Exploring The Science of Transsexuality
Through Knowledge, Justice…
 This blog is on the science of transsexuality and transgender sexuality, including aspects of sexual orientation. The blog also explores socio-political themes where appropriate. There are many myths and misunderstandings about transsexuality and transgender people. Our scientific understanding of the transsexual phenomena has increased and dramatically improved over the past sixty years, yet much of what is available in popular literature is misinformation and disinformation. Much of what the public, including transsexuals and transgender people themselves, believe about the etiology and epidemiology of transsexuality is based on wishful thinking on one hand and deliberate distortions on the other. Worse, many cherry-pick among the scientific papers, choosing those that, in isolation, appear to support a given thesis. Many people have read misinformation and disinformation regarding the science, denying, decrying, and even weaponizing the science, often in emotionally inflammatory language (including vicious attacks on the characters of scientists and educators), that makes its rounds in the echo chamber of the web and social media. Indeed, there are fora that will instantly ban any who discuss this science in any truthful way. This blog is an attempt to correct this situation.
This blog is on the science of transsexuality and transgender sexuality, including aspects of sexual orientation. The blog also explores socio-political themes where appropriate. There are many myths and misunderstandings about transsexuality and transgender people. Our scientific understanding of the transsexual phenomena has increased and dramatically improved over the past sixty years, yet much of what is available in popular literature is misinformation and disinformation. Much of what the public, including transsexuals and transgender people themselves, believe about the etiology and epidemiology of transsexuality is based on wishful thinking on one hand and deliberate distortions on the other. Worse, many cherry-pick among the scientific papers, choosing those that, in isolation, appear to support a given thesis. Many people have read misinformation and disinformation regarding the science, denying, decrying, and even weaponizing the science, often in emotionally inflammatory language (including vicious attacks on the characters of scientists and educators), that makes its rounds in the echo chamber of the web and social media. Indeed, there are fora that will instantly ban any who discuss this science in any truthful way. This blog is an attempt to correct this situation.
Learning an unpleasant truth is better than believing a comforting lie – Don’t let the “tribe” tell you what to think – Trust only evidence, not vehemence –Data, not denial
All information found in this blog is supported by peer reviewed science and referenced (cited) in essay posts covering a given topic found on this site. Many topics are interwoven with other topics, as they are interlocking issues. Please explore the entire site for a full explanation of each topic.
I recommend that one read the first several entries in the FAQ as an introduction and jumping off point via the links provided. One can find a bibliography for this blog if you wish to quickly find papers of interest. You may wish to review the Glossary if a word is unfamiliar.
Remember as you read this site; Transsexuals and transgendered people are good people, worthy of our respect, and even of our admiration. Nothing in this material is meant to imply otherwise. If you are a transsexual or transgendered person: You have value as a human being. You have the right to be respected, valued, and even celebrated as the gender to which you identify and aspire regardless of etiology.

Excerpt From My Memoire: A Life In Transition
It won’t work out
It started the first weeks of my Junior year. I met the “Terrible Trio”, Barbara, Liz, and Barby, three freshman girls who had been friends since Kindergarten. Barbara was clearly the leader of the three. Somehow her outgoing nature made it possible for her to make instant acquaintances of everyone. She latched onto me the first day! She got the notion into her head that she was going to have me as her boyfriend. If you know Barbara, you just know that she gets her own way. She was forever telling everyone that she and I were an item. This presumptuousness amused me greatly at first, but began to pall. She even started writing romantic love poems and gave them to me, hand written, in a ‘blank book’. Now for some silly reason this made Cassie very jealous. Never mind that I wasn’t really going with Cassie, just friends with her, she was not going to let Barbara have me. Never mind that I had zero interest in going with Barbara, she was determined that I would. It was funny in retrospect but at the time this was very distressing. One morning, just a few weeks into the school year, they squared off for a shouting match in the hallway. I was so distressed by the spectacle, (over me? why? Nobody was going to win me anyway!) I just sat down on the concrete and hung my head in exasperation. Barby later recounted to me that that was the moment that she fell in love with me, head over heels, no turning back.
Apparently Barbara has a very good heart because when Barby told her this, Barbara turned all of her energy into helping win me for Barby instead of herself. Barbara and Liz made sure that Barby was sitting next to me, all of the time. Barby began to ‘puppy dog’ me. I couldn’t turn around without her there. I ignored her completely. This went on for weeks.
My mother insisted that my sibs and I have a Halloween party that year. She said we were not to be going out and doing anything like what she suspected had happened the year before. (I seem to recall there might have been something about my brother Mark being seen near where eggs landed on a patrol car over on Edith Avenue as it crossed the bridge over the creek?) She said that we each could invite some friends over that night. I invited a few friends (all girls, no boys, as they all had other, less “wholesome” plans) including Cassie, Kathy, Beep (short for Beatrice P.), Barbara, Liz, and Barby. Well, I found out later that Barbara had gone around telling everyone but Barby not to go. So come Halloween night I was disappointed to find that only Barby had come. I was actually hurt, Barby was not my favorite. But she was still a nice kid, if a little too ‘puppyish’. We pulled taffy together, played Frisbee and ping pong in the garage (silly three car, three door monstrosity that virtually hid the rest of the house from the street), bobbed for apples, and swapped tales of previous Halloweens. Barby was ecstatic. I was actually paying attention to her!
But back at school… I ignored her completely!
A number of more weeks go by. One night I get a call from Barbara. I remember the conversation very well. I was very distressed by it on several levels.
“Did you know that it was Barby’s birthday today?”
“No, I didn’t”
“She had a birthday party today.”
“Oh,” I said, wondering where this was leading to and why it should concern me.
“Yes, and she was crying at her own birthday party!”
Now I was feeling sorry for her. I did not feel close to her but I did like her and would never have wanted to see her feeling blue. I asked very concerned and perplexed, “Why? Why was she crying, I don’t understand?”
“She was crying over you!” She burst out in a very accusatory tone, “She was crying because you won’t even notice her! You know that she’s in love with you and you treat her like dirt!”
Now I felt very defensive. I had done nothing to encourage Barby. On the contrary, while I was never cruel, I had irritatedly snubbed her, repeatedly.
“Why won’t you be nice to her?”
“I am not interested in her.”
“Why not? She loves you! Why can’t you just be nice to her? Why can’t you just take her out some? Why can’t you just take her to the Christmas Dance?”
“Because it would never work out! That’s why!!”
“Give me a good reason!”
“Look, it just wouldn’t work out!” I was thinking, yeah, right. I’m going to just tell Barbara, the biggest gossip on campus, that I’m not attracted to girls but I am to boys, Yep, and I’m going to tell her that I’m already researching how I’m going to get sex change surgery!
“I’m not going to get off the phone until you tell me why you can’t just take her to one lousy dance?!”
We went in circles for half an hour with me telling her that it wouldn’t be a good idea and would she please just drop it. I knew from prior experience that just hanging up wouldn’t do. She would call back. If I left the phone off the hook she would just give me hell the next day. Barbara is very persistent. Finally in exasperation I caved in, “Alright, alright! I give up. I will invite her to the Christmas Dance if it will make you happy.” Since I loved dancing, I actually wanted to go to the Christmas dance. But it was the one dance a year that one couldn’t go stag. Though it wasn’t a school rule, it was socially required that you go with a date. I had thought I would go with one of my friends, perhaps Cassie or Kathy, if either didn’t have a real date lined up. I knew Beep had a steady boyfriend, so she was out. So, if I had to have a date, it might as well be Barby.
Having gotten her way, Barbara’s tone instantly turned friendly, “Oh, she’ll be so happy! You won’t regret it, you’ll see.”
“OK, OK, What’s her number?” I said resigning myself.
“Well, she isn’t home tonight, she’s baby-sitting. But I have that number too.” She hung up after giving me the number.
Feeling like I had been had, I dialed the number. “Hello?” a very uncertain voice answered. It was Barby, and it did sound like she had been crying and sniffling. My heart broke. I didn’t want to be the cause of that. And I didn’t want to be her ‘boyfriend’. But I told myself, just one date, just one date. “Hi, Barby, it’s XXX.” I heard a sharp intake of breath. I had definitely surprised her. Well, I thought, no sense in delay, “Would you like to go to the Christmas Dance with me?” I could clearly hear her stifle a squeal as she began jumping up and down. I groaned inwardly, what have I gotten myself into?
“Yes, Yes, I would love to!”
“Good then, I’ll see you tomorrow, bye.”
“Bye.”
I could hear her give full throat to that previously squelched squeal before the receiver actually made it to the hook. I just chuckled and shook my head.
I took her to the Christmas dance, bringing her a very lovely corsage, as the dance was a formal affair. I felt like I was humoring a small and precious child. Afterwards, she still puppy-dogged behind me, but I no longer snubbed her. She even tagged along by signing up for the same science class the next semester. It forced me to have to spend a lot of time tutoring her, to keep her from falling hopelessly behind. I learned that she was actually a very sweet and generous soul. She volunteered at Agnew’s State Hospital, helping the mentally retarded. She was very happy, because I was her “boyfriend”. It stayed that way for months, until I began to trust her and finally told her that I was transsexual that next summer, the summer I had the nanny job. I had to tell her, as she was beginning to push for sexual intimacy, something I just couldn’t give her. She reacted with deep disappointment and discomfort yet with sympathy. She wanted to keep me as her “boyfriend”, and only slowly stopped tagging after me. It took six months to convince her I was serious. After that she went from being a kid that I was humoring to being a good friend.
I finally came out to Barbara at next year’s Christmas Dance, my Senior year. That is when I told Barbara why it hadn’t worked out!
Comments Off on Excerpt From My Memoire: A Life In Transition
Family Memories

My father died a year ago. I’ve been thinking of him a lot lately, missing him. So I thought I would share some memories of him and my family, a bit more detail than I shared here in the past in my “About” page.
My father was a very loving and devoted father. He had very high aspirations and expectations for all of us. He spent many hours encouraging us in school matters and tutoring us in various STEM and business topics. My siblings and I were all expected to do well in life and all of us did. I became a high tech executive and entrepreneur. the older of my two brothers became an engineer, then next became a doctor, our sister, the youngest, became a business woman. She inherited our father’s last business and continues to run it today.
My parents separated and divorced when I was in high school, around the same time I began to socially transition and was officially diagnosed as transsexual and accepted into the Stanford Gender Dysphoria Clinic’s program in 1975. Each remarried later. But my mother remarried just as I was leaving home at 18, as “requested”. Though I was already living full time as a girl, my mother insisted that I wear a men’s suit and tie to her wedding to her new husband so as not to “embarrass” her.
As teens, our families freaked out when they learned that the older of my two brothers best friend, Don, and I were lovers. Don had been a frequent and welcome guest at my mother’s house until that discovery. He was devastated when that was no longer the case. Under pressure from his father, he broke off our relationship.
Some years later, the younger two of my three siblings had gotten married with the collusion of ALL of my family, to keep it secret so that I wouldn’t show up uninvited. I have literally never met their spouses. The older of my two brothers told me it was because they were afraid I would dance with a man at the receptions, further embarrassing them.

I met Jeff the summer of 1997. We’ve been an “item” ever since. In early ’98 he proposed. I made a point of introducing him to both of my parents, on separate occasions, before then, as I felt we were headed in that direction. My mother pulled me aside to ask me “Does he know?”
When visiting my father’s house in southern Oregon with Jeff, my father surprised me by refusing to let Jeff and I stay together in his guest room. We had to find a motel room for the night. Since I knew for a fact that my father would have had no qualms about me sleeping with a woman, as he was often trying to get to do so since I was a teen, falsely believing that it would “cure” me, it was clear that it was homophobia. At that point, he still hadn’t gotten to the point of admitting that one of his two brothers was gay.

Jeff and I had a long engagement, a bit over a year, during which I planned a small and very elegant garden wedding at a nearby, Wine Country, Bed & Breakfast. I rented the entire B&B, ordered flowers, cake, catering, and bought airline tickets for my Matron of Honor and another friend. I invited all my siblings; the younger two didn’t even bother to respond. My Uncle, a Methodist minister, and his wife planned to drive out to attend and to officiate. The older of my brothers agreed to let his son to be the ring bearer. Liz was to be one of the flower girls. My father said he would come, perhaps even walk me down the isle, while his wife guaranteed it. Turned out that her mother lived nearby so they would be staying at her place.
My mother offered to help me find my wedding dress. On the day she drove up to Jeff’s house to meet up to start shopping, I described my dream dress in detail, nothing else would do. She sighed, believing that I was going to be a bridezilla. But I was optimistic. We went to the local mall, to the main department store with a bridal department. I walked in, headed for the ‘sale’ rack, pulled open the dresses in my size… and there it was, exactly as I had described. The dress had some minor flaws and tears given that it had been on the show room, so my mother negotiated on the price, which I knew she would, being the reason I agreed to go shopping with her. Later, I repaired all the issues by hand sewing to near perfection.
So, onto the wedding. But instead of my writing about it, please allow me share what, Magdalena, my Matron of Honor, wrote about it. But let me add, that because of events that surrounding the wedding, I haven’t had any contact with my mother or my two younger siblings since, that’s 25 years now. While Jeff and I are still happily married and love each other very much.
Matron of Honor…
by Magdalena
I wish that I could say that from the first moment I heard about Jeff and Candice’s relationship that I was supportive. That wasn’t the case. While I trust Candice’s judgment, there was a part of me that wondered, “Is this guy a user, a loser, a freak, or all of the above in some sort of David Lynch inspired combination?”
I get ahead of myself. Let me start by saying that one of my favorite “pop” songs is Winter, by Tori Amos specifically because of this lyric:
“When you gonna love you as much as I do
When you gonna make up your mind
Cause things are gonna change so fast
All the white horses are still in bed
I tell you that I’ll always want you near
You say that things change my dear”
This song reminds me of Candice, because while she has an incredible capacity to love, at times that capacity does not extend to herself. In addition, I am a woman who has experienced abuse. Unfortunately, this is something Candice and I have in common. Understanding that a history of abuse makes it more likely that you will end up in another abusive relationship makes me evaluate my own relationships and those of my friends with a careful eye.
So when Candice called to share with me that she was a: getting married and b: asking me to be her Matron of Honor, I was happy for her, genuinely happy, but cautiously so. I remember thinking, Dear gods, what will I do if I have to, out of love, say, “Candice. I love you. No. By all that is holy, no.”
Luckily, within moments of meeting Jeff, I saw that she had found, not just a good man, but a wonderful, responsible, intelligent, loving man. A man that would love her as she deserved to be loved. I watched not only an unaffected and completely genuine love for, and cherishing of, my dearest friend, but I saw that for Jeff, giving that patience and love was a way of life. From the cats that shared his home, to his immediate gentle concern for my young daughter, Jeff is the kind of man that showers all around him with gentle good humor, kindness, and compassion.
At that point, I turned my sights to the next hurdle.
Candice’s mother, the wire monkey woman.
Please understand, Candice’s mother is a lovely woman. If you ever meet her, she will be polite to your face. Excruciatingly, terrifyingly, absolutely polite. She will carefully assess your family and social class, (while refraining from checking your teeth… she is a lady, after-all!) and then she will graciously engage you in a perfectly correct, yet entertaining conversation eminently appropriate to all of the above and the occasion. Miss Post and Martha Stewart have nothing on Candice’s mother.

I should have been able to get along with the mother of the bride. In fact, we didn’t have an out and out confrontation. I think it would be more accurate to say that she and I treated one another like dignitaries from sovereign nations – both of which had thermonuclear weaponry. I’m sure at first, she was even comfortable with me; I was raised in a “good” family (outwardly anyway). I know when to nod and smile, I know the difference between a shrimp fork and a salad fork. I understand that proper Methodist etiquette for any disaster is to bring a casserole along with just the right amount of sympathy, nothing outlandish, mind you, a simple, “Ah, now that is too bad” will suffice.
However, I did make one immediate tactical error. I admitted that I absolutely love and accept Candice. We are more than friends. This is a woman I consider the sister of my heart, one of my dearest friends, and the person I have chosen to care for my children should I ever be unable to. While I’m sure it was expected that I, as the Matron of Honor, would be gracious in respect to the nuptials, I’m also quite sure that my unqualified support was considered a bit unseemly.
My second tactical error came when I found a charming group of women who enthusiastically offered to care for my six month old while I attended to last minute details. Any new mother can attest that when a group of obviously intelligent, clearly compassionate caregivers offer to watch your child for you – for free, no less, you jump at the opportunity. Clarity had spent less than ten minutes with her adoring new friends when I was approached by MoB. She took me aside, (What, did you think she would cause a SCENE? Tsk. Tsk. Tsk. We do not do such things.) Honestly, when she came up to me I thought a small Wedding Disaster™ had occurred, perhaps the flower girl had socked the ringbearer to kingdom come, or maybe someone had picked up the wrong cake and we were now faced with a “Happy Bar Mitzvah, Bart” cake instead. As an experienced Matron of Honor, I was well prepared for those types of Mother of the Bride disasters. However, I was dumbfounded when she kindly said to me, sotto voice, “You really don’t want to leave the baby with THOSE people do you?”
…
I will admit. I was distracted. I was not quick on the uptake. My first thought was, “With a pianist? With women in hats? What kind of people is this woman talking about?” Her lip curled. Yet, remember, MoB is a lady. Ladies do not openly call other ladies “Stupid idiots” in public. She gestured again towards where my daughter was being lovingly cradled and entertained with classical piano.
I was stunned as it hit me like a slap to the face. Those people? The ones she did not feel were fit to even hold my daughter… were trannies. In that moment, I have to admit, I began to hate this woman. I hated the fact that she could not, no, she flat out refused to see any of this group of women for what they were – talented, kind, loving individuals. I hated the reality that she considered “them” a class so poisonous that she felt my baby was somehow in danger — From what? A lipstick kiss? Being spoiled? Having a cultural experience?
Was she afraid that someone would say the T word in front of Clarity? Was she concerned that somehow Clarity would “get the gay” ? Whatever her fear was, whatever anger she had, I could not, nor would I ever participate in it. My exact words to her are lost in my memory at present, but I will assure you that I did not say what I wanted to, “Who the FUCK are you, you pompous BITCH to presume that I would ever leave my child with someone I thought was inappropriate.” If my daughter is being cared for by another person you may presume that I feel that person is perfectly safe, sane, and appropriate as a caregiver for that situation. Unlike some, I do not consider transsexualism a deadly contagion.
Another surreal moment for me as we prepared for the wedding happened as I was making small talk with MoB. As mothers often do, we began sharing stories from our children’s childhood. I found myself aghast as Candice’s mother said, sadly, “You know, (deadname) was such a good boy until he was seventeen.”
How was I supposed to answer this? What do you say to someone who is so self righteous that she believed that she was entitled to sympathy. Sympathy for what? Not accepting her daughter? For torturing her child with rejection? There are many things I would dearly love to give to Candice’s mother. Sympathy is not one of those things.
I do not want to leave anyone with the impression that I regretted meeting Candice’s mother. I appreciated the chance to have had a taste of the civil ugliness that Candice lived with every day of her childhood and adolescence. I had the opportunity to see just how much hatred Candice experienced in her own home and just how much strength of character it took to leave that hatred behind.
I did, however, decide that I would place myself squarely between Candice and her mother to deflect any possible nastiness. Frankly, as a person who grew up Irish Catholic, married a Methodist, and then became Wiccan, I am more than capable of handling a prissy, uptight, bigoted bitch. With the help of another friend, and using Candice’s nephew, Matt, as an unwitting accomplice, we occupied Dianne quite effectively with many small, “Oh, dear… do you really think Matt should be doing that?” episodes, thus making sure that she had little time to dig at the bride.

One of my most treasured memories of that afternoon was helping Candice dress for her wedding. It may sound trite, but she was radiant, beautiful bride. The sun streamed into the bridal suite at the Gravenstein Inn making the beads on her dress shimmer and sparkle. The flowers I pinned into her hair smelled sweet and old fashioned, and I remember having to brush tears away as I fastened a blue band around her wrist, my old ring dangling from it. Brides wear something old, something new, something borrowed and something blue for luck, but that day it was clear to me that Candice and Jeff didn’t need luck, they had each other and that would be more than enough.
As Candice made the final adjustments, I went downstairs to assure myself that Candice’s father was going to walk her down the aisle as agreed. I steeled myself ahead of time, prepared for anything after having met Dianne.

Candice’s father is the kind of man that could easily explain to you the inner workings of a nuclear power plant, how to best secure the resources of a venture capitalist, or how to make an industrial strength solvent from ingredients found in your kitchen. More importantly, whatever he’s sharing with you is made interesting by the fact that this brilliant man can actually communicate. Perhaps he wasn’t the perfect father when Candice was younger. There were probably many things he could have and should have done differently. Yet on that May afternoon, he was warm, he was kind, and he was there to support his daughter. For that, I loved and respected him.
One might think that once the wedding was over, the bride and groom off to enjoy a romantic dinner, and guests dispersed, that any opportunity for drama would have evaporated. One would be wrong. In the evening, after a long and tiring day, I sat down with Candice’s (adopted foster) daughter, Elizabeth, to chat. It was then that I discovered that Gilroy’s answer to a Stepford wife wasn’t done spreading poison.

I listened with growing fury and disgust as Elizabeth shared her experience with her grandmother, Dianne. Apparently, she asked Elizabeth something along the lines of, “So now that Jeff is in your family, which one are you going to call Daddy? Jeff or Candice?”
I was absolutely stunned. Truly, I knew the woman was a sick, vile, twisted bitch. I honestly didn’t think that she would go so far as to use her granddaughter to strike at her daughter. To this day, it makes me sick to my stomach when I think about the bitterness and the ugliness that would twist a person’s heart to the point where they would say something so utterly cruel, confusing, and inappropriate to a child.
There are no words.

As I look back on that time, I realize one important thing. People like Candice’s mother do not like being proven wrong. In fact, fundamental to their lives is a smug insistence on just how “right” they are. Once, years prior, this judgmental wire monkey of a woman had told Candice, “No man will ever love you.” On that day, it was abundantly clear in more ways than one, that she was wrong. Rereading this piece, I do not want to leave anyone with the impression that a bitter self righteous woman dominated my best friend’s wedding. She didn’t. Thankfully, Janeen and I were able to insulate Candice from the attitudes of hatred and prejudice that she grew up with if only for that one day. If we had no other role, I am glad that we were able to fulfill that one. The lesson that I wish Dianne had learned was that the wedding wasn’t about her. In fact, nothing about Candice’s life was, or ever has been, about this woman. Perhaps if she could see that she’d be a little more accepting and a little less judgmental. Regardless, it was a beautiful day and everything a wedding is supposed to be – a commitment between two people who truly love, honor, and accept one another and I feel very honored to have been a small part of it.

Comments Off on Family Memories
Australian Study of Gender Dysphoric Teens
We have another new study of teens referred to a gender dysphoria clinic. The results are very similar to that from the UK. Approximately 6% “desisted” BEFORE or DURING the evaluation period, that is, before any medical transition services were begun. As so many have pointed out, this shows that not all teens referred to a clinic are actually gender dysphoric, either due to outsiders mistaking gender atypicality or due to teens falsely claiming to be “trans” or “non-binary”, until “shit gets real”. The interesting part is that only two (~1%) of the nearly two hundred teens who began any medical transition services “detransionted”.
These studies show that transsexual teens are stable in their gender dysphoria and that our current diagnostic and treatment modalities are serving them well.
Further Reading:
Transsexual Teens In UK Gender Dysphoria Treatment
Reference:
Cavve BS, Bickendorf X, Ball J, et al. Reidentification With Birth-Registered Sex in a Western Australian Pediatric Gender Clinic Cohort. JAMA Pediatr. Published online March 04, 2024. doi:10.1001/jamapediatrics.2024.0077
Comments Off on Australian Study of Gender Dysphoric Teens
Hypothesis: Do Gynandromorphophiles (Chasers) Over-perceive Sexual Interest From MTF Transsexuals?
Ask any straight woman how many times straight men have misperceived, or other “over-perceived” sexual interest from them when they were merely being friendly. There is a documented bias in heterosexual male perceptions of women’s interest in them. Interestingly, this may have come from evolutionary history, as Haselton explains,
“Mammalian males and females faced different selection pressures during their evolution. According to Trivers theory of parental investment, the sex with a greater obligatory investment in reproduction, typically the female, should evolve to be choosy in selecting a mate. The sex with lower obligatory investment, typically the male, should evolve to be less choosy and to be highly competitive for access to members of the high investing sex. — The logic of parental investment theory suggests that for males the fitness costs of missed sexual opportunities will often be greater than the costs of some lost time or effort wasted on unsuccessful courtship. Within a given population, males who miss reproductive opportunities with some regularity will be out-reproduced by males who do not. This is not true for most females. The reproductive variance among females, including human females, is typically far more constrained because of limits imposed by the time and energetic costs of gestation and offspring care (Trivers, 1972). At any point in time, females may receive low to non-existent marginal reproductive benefits of additional mating opportunities because of current pregnancy, lactational amenorrhea, or because they have ready access to another fertile mate (Symons, 1979). Although courtship effort is costly for males, in the currency of differential reproduction these costs will often pale in comparison to the costs of missed mating opportunities.”
The is over-perception bias does NOT occur in straight women. Regardless of whether the phenomenon is an evolved one or a result of socialization in a patriarchal society, the differential bias is constant across different societies, leading to stronger weight to in-born cognitive processes being sexually dimorphic. Again, from Hazelton,
“Experimental evidence suggests that human males may indeed possess this bias. In laboratory experiments, photographic and video stimuli experiments, and minimal experiments using written scenarios or brief descriptions of dating cues, researchers have compared men’s perceptions of women’s sexual intent with women’s perceptions of women’s sexual intent. Men’s estimates of women’s sexual intent are consistently higher than are women’s. This pattern holds when men’s perceptions are compared to women’s perceptions of their own sexual intent and when compared to women’s perceptions of third-party women’s intent. When women’s interpretations of men’s behavior have been examined, there has been little evidence of bias.”
This phenomenon in gynephilic men led to the question, does this phenomena exist in homosexual or bisexual men and women? A very recent paper by Moran explored this, as stated in their abstract,
“Research on perceptions of sexual interest has documented the tendency for men to overperceive sexual interest (i.e., to perceive a social signal as indicating more sexual intent than the actor intended). However, this work has almost exclusively focused upon these dynamics among heterosexual individuals. Thus, the current set of studies aimed to understand how perceptions of sexual interest manifest among lesbian, gay, and bisexual (LGB) women and men. In Study 1 (N = 85), LGB women and men nominated behaviors that signal sexual intent. Using an act nomination approach, LGB women and men tended to nominate behaviors similar to those nominated by heterosexual women and men. In Study 2 (N = 43), gay men reported acts that were representative of their own and other gay men’s sexual interest. Consistent with previous work—by comparing perceived self-reported versus others’ sexual intent when engaging in specific behaviors—we found no evidence for a sexual overperception bias in gay men, albeit in a small field study. In Study 3 (N = 307), using a gender-by-sexual orientation design, heterosexual and LGB women and men reported previous experiences in which their friendliness was sexually misperceived. Bisexual women were less likely than other groups to report their friendliness being misinterpreted as sexual by other bisexual women and/or lesbians.”
This result suggests that this phenomenon of over-perception bias is only to be found in gynephilic males. This in turn leads me to posit a new hypothesis, that gynandromorphophilic males (chasers), who we also know from research are also gynephilic, also exhibit this over perception bias when interacting with transwomen. It is important to know that gynephilic and (pseudo) bisexual transwomen are both autogynephilic and gynandromorphophilic. As such, they also have exhibit this over-perception bias. I would invite sexologists to explore this hypothesis, to test it experimentally and using natural events surveys.
For myself, I strongly believe this hypothesis will have experimental support. In the mean time, I will share some anecdotes and community observations to support my personal belief. In the “Further Reading” section below, I link to essays in which I experienced such. It may not be science, but it may help to explore the phenomenon in the wild, so to speak.
In one documented example, two very well known transwomen exhibited this phenomenon. Andrea James, in her effort to smear Dr. Anne Lawrence, recounted on her website, in vilifying tones, an event during the time when they had been on friendly terms, in which Dr. Lawrence over-perceived James’s putative interest in having sex with her. There were no negative repercussions to the error, but James attempted to paint Lawrence in a negative light.

In addition to over-perceiving sexual interest directed towards oneself, the research above showed that gynephilic males also over-perceived sexual interest by women when observing interactions with other men. I strongly believe that this has operated in my own life, with silly consequences where people falsely believed that Dr. Joy Shaffer, my college roommate and political ally, and I were lovers, when we never were, and have promoted this false belief in the transsexual community for years.
Further Reading:
The Love That Can’t Pronounce Its Name
Cognitive Dissonance and Vector Transform Miscalculations in Transgender Tensor Space
References:
Abbey, A. (1982). Sex differences in attributions for friendly behavior: Do males misperceive females’ friendliness? Journal of Personality and Social Psychology, 42(5), 830–838. https://doi.org/10.1037/0022-3514.42.5.830
Martie G. Haselton, “The sexual overperception bias: Evidence of a systematic bias in men from a survey of naturally occurring events”, Journal of Research in Personality, Volume 37, Issue 1, (2003),
https://doi.org/10.1016/S0092-6566(02)00529-9
Bendixen, M. (2014). Evidence of Systematic Bias in Sexual Over- and Underperception of Naturally Occurring Events: A Direct Replication of Hazelton in a more Gender-Equal Culture. Evolutionary Psychology, 12(5), 1004-1021. https://doi.org/10.1177/147470491401200510
Moran, J.B., Airington, Z., McGee, E. et al. (Mis)Perceiving Sexual Intent: A Mixed-Method Approach Investigating Sexual Overperception Across Diverse Sexual Identities. Arch Sex Behav 53, 511–524 (2024). https://doi.org/10.1007/s10508-023-02748-7
Comments Off on Hypothesis: Do Gynandromorphophiles (Chasers) Over-perceive Sexual Interest From MTF Transsexuals?
Old News: MRI Brain Scans Show Men and Women Are Different
Today, news outlets around the world breathlessly announced that a study at Stanford University showed that AI can look at MRI brain scans and determine their sex with 90% accuracy. The issue is that though the mainstream press is acting like this is a new and amazing development, it is actually old news. Scientists have been publishing studies regarding sexual dimorphism of the human brain for years, including those based on MRI research… and even a few based on AI training and testing of those very MRI brain scans. We have known that the human brain is sexually dimorphic and that one can determine the sex of the individual from their brain scan at better than 90% accuracy for over five years, as I previously wrote about in 2017.
Update 2/20/24 in the afternoon: I finally was able to access the citation for the paper as it just published. I am attempting to obtain a copy, as the devil is always in the data, not the abstract.
Update 2/21/24 in the morning: Dr. Menon, the corresponding author of the paper emailed to me an offprint of the paper. I’m currently reading it with great interest. The press really didn’t represent what is novel about this study, specifically that the researchers used a “movie” instead of the usual “snapshots” of the fMRI as the imput to an XAI, that’s an “Explainable Artificial Intellegence” algorithm instead of a ‘black box” AI. I will write more as I analyze and critique the results.
Further Reading:
Further External Reading:
https://www.eurekalert.org/news-releases/1034374
https://nypost.com/2024/02/20/lifestyle/mens-and-womens-brains-do-work-differently
Reference:
Ryali, S., et al, “Deep learning models reveal replicable, generalizable, and behaviorally relevant sex differences in human functional brain organization” PNAS (2024)
https://doi.org/10.1073/pnas.2310012121
Comments Off on Old News: MRI Brain Scans Show Men and Women Are Different
The REAL Takeaway From The CDC Study On HIV/AIDS In Transwomen
The CDC is clueless.
Seriously, they are. They conducted a study in seven urban areas of Male-To-Female transsexuals, regardless of surgical status, asking about HIV status along with a number of other questions, but like so many who have no clue as to the Two Type Taxonomy, simply assumed that everyone who is “trans” is in the same etiological taxon, with similar behaviors. Clueless.

Because of this, they seem surprised that unlike in the gay and bisexual male population, black and latina transwomen were more likely to use PrEP medications (anti-viral drugs that protect one from HIV) than white. Of course they are! As was documented by Nuttbrock, most white transwomen are heterosexual autogynephilic (AGP) while most black and latina transwomen are Homosexual Transsexuals (HSTS). White AGP transwomen are simply NOT at the same high risk of getting HIV as HSTS of any race and they know it, thus are less likely to use PrEP.
Only 11% of the CDC’s study respondents were white, which is dramatically lower than the percentage at the national level. This indicates that the study, given its urban catchment and the networking effect of how the subjects were recruited from other subjects, this study was very likely mostly of HSTS transsexuals. This is born out by the fact that 77% reported receptive anal sex during the past year — and 55% reported condomless anal sex — but only 14% reported vaginal sex with women.
So, why did the CDC researchers ignore the two type taxonomy and fail to report that the single highest risk factor for HIV infection in the United States among transwomen is being an HSTS and that AGP transsexuals are at much lower risk? Healthcare workers need to know this differential risk factor.
The write-up did acknowledge that the study was limited by the fact that they had not captured those that would likely be at lower risk… but failed to note that that difference came from the disparities experienced between AGP and HSTS transsexuals.
Further Reading:
Nuttbrock data on HSTS/AGP ratios by race
Further External Reading:
Reference:
Comments Off on The REAL Takeaway From The CDC Study On HIV/AIDS In Transwomen
Men And Women Walk Differently: The Challenge For Transsexuals
Decades ago, when I was just turned 13 years old in the summer of 1970, the Kinks put out a new hit song, “Lola”. It was a revelation for me. It told me that not only was I not alone in the world, but that there were men who would find me attractive and love me. I loved the song and turned up the volume on my pocket transistor radio every time it played. One of the verses is, “Well, I’m not dumb but I can’t understand, Why she walked like a woman but talked like a man. Oh my Lola.” The song referred to the well known tendency of homosexual transsexuals (HSTS) to have a naturally feminine gait.
This brings us to the current essay regarding sexually dimorphic walking gaits and the ability of observers to identify the sex of the walker from that gait. Scientists have been studying this in the late 1960s with some interesting results. In order to study this phenomena in isolation from other gendered cues, they used video of people walking where the only objects visible were reflective tape adhering to dark clothing at the joints, etc.

It creates an array of white dots that represent the human body in schematic form. Interestingly, observers can still perceive this as a person walking as though on a treadmill towards them. The perception of the walker’s sex from this very limited information is gathered and analyzed statically. Averaging the responses, the observers can tell the sex better than random (50%) at 66%. However, asking the observers how confident they were in their judgments yields a positive correlation in which those perceptions that they were confident about were more correct, with accuracies of 90%. This suggests that not only is walking gait sexually dimorphic overall, but that there is also a range of gaits between walkers, where some more pronounced than others. Interestingly, using machine learning algorithms, the overall accuracy was in the range of 85%. This supports the observation that walking gaits are indeed sexually dimorphic.
There were still questions, of course, about what was being used to judge the sex of the walker. Were they getting some cues from structural differences that the reflective tape dots captured? (Hip to Shoulder Width Ratio?) If not, what in particular about the gate was the strong gendered cue? To answer that, artificial walkers, computer simulations of the white dots, were created from the motion analysis, in which the structural cues could be manipulated separately from movement cues. From this they discovered that structural cues had some effect, but was swamped out, over-ridden by the movement cues. This is both good news and bad news for transsexuals. Good for HSTS, bad for AGPs.
So what motion cues lead to sex attribution? Interestingly, cultural references got it right. Masculine men “swagger” and even “lurch”, move their shoulders and with it their heads from side to side while feminine women hold their shoulders and heads nearly constant while their hips may sway from side to side while also tipping the angle of their hips. Because their heads do not move side to side very much, they will appear only to bob up an down instead. In both homophobic and camp representations of feminine gay men, they “swish” and “sashay” along as they walk. This last is NOT a performance, but a natural product of a feminized brain.
However, runway fashion models accentuate this sexually dimorphic gait when modeling designer clothing by wearing very high heals and carefully stepping counter to their stride, actually crossing over each foot, to cancel any side to side motion of their shoulders and head while simultaneously increasing the hip sway and tip.
Similarly, for MTF HSTS vs. AGPs, their is a natural difference in their gaits, one in which HSTS appear feminine and AGPs appear masculine. Before social transition, this causes HSTS to be recognized as gender atypical and in many cases, targeted by homophobic bullies. Post social transition, this very gait helps them pass as female. While for AGPs, post-social transition, their walking gait adds one more masculine signifier that leads to them to be “clocked”.
As a reminder, sex attribution is biased toward male by about five to one. It takes five feminine attributes to counter each and every masculine one. And for individuals who are clued into the existence of transgender people, it may be even higher. AGPs can learn to mimic a feminine gait, but it takes effort and practice… and coaching. Most never do in my experience.
Further Reading:
References:
Mather George, Murdoch L., “Gender discrimination in biological motion displays based on dynamic cues” Proc. R. Soc. Lond. B.258273–279 (1994) http://doi.org/10.1098/rspb.1994.0173
Viswadeep Sarangi, Adar Pelah, William Edward Hahn, Elan Barenholtz, “Neural and Neuromimetic Perception: A Comparative Study of Gender Classification from Human Gait” in Journal of Perceptual Imaging, (2020), pp 010402-1 – 010402-11, https://doi.org/10.2352/J.Percept.Imaging.2020.3.1.010402
Sarangi V, Pelah A, Hahn WE, Barenholtz E. “Gender Perception From Gait: A Comparison Between Biological, Biomimetic and Non-biomimetic Learning Paradigms.” Front Hum Neurosci. 2020 Aug 27;14:320. doi: 10.3389/fnhum.2020.00320. PMID: 33117137; PMCID: PMC7493679.
Kozlowski, L.T., Cutting, J.E. “Recognizing the sex of a walker from a dynamic point-light display.” Perception & Psychophysics 21, 575–580 (1977). https://doi.org/10.3758/BF03198740
Comments Off on Men And Women Walk Differently: The Challenge For Transsexuals
Insights Gleaned From “Detrans” People
A new study in the January 2024 issue of the Archives of Sexual Behavior, but published online the previous month, NOT behind a paywall, looked at “Detransistioners”. It was written by some very well known sexologists who who have studied transsexuals and transgendered people, Littman, O’Malley, Bailey… From it we can glean some interesting tidbits of knowledge, some of it likely NOT what some of authors would have wanted to find.
First, is the incredibly small number of subjects at only 78 individuals in spite of having trolled the internet to find them, most having come from the “detrans” subgroup on Reddit. This is snarkily amusing in that I can recall being told that there were “thousands” of “detransitioners” on that subgroup by transphobes insisting that most people who transition later detransition. To this, I would point to my essay, in which I list a number of studies that show that such is actually quite rare. Even the authors of the paper tried to explain that away, as being “old data”, before the recent explosion of “Rapid Onset Gender Dysphoria” (a term that the first author of this study coined a few years back). Further reducing the number of subjects that we can honestly label, “detrans”, is the fact is that 25 of that 78 had never even “transitioned” in the first place, leaving only 53 actual detransitioners. Of those, only 18 had had any surgical procedures.
Given that we have studies, some published in the past year alone, involving literally many thousands of post-operative transitioners, looking at the number who regretted surgery and detransitioned shows that incidence rate is only 0.15%, finding only 18 subjects who had detransitioned after such procedures after scouring the internet in the most likely places is quite reasonable and does NOT represent a huge rate. In fact, it supports the conclusion that such post-op regret and detrans is indeed rare.
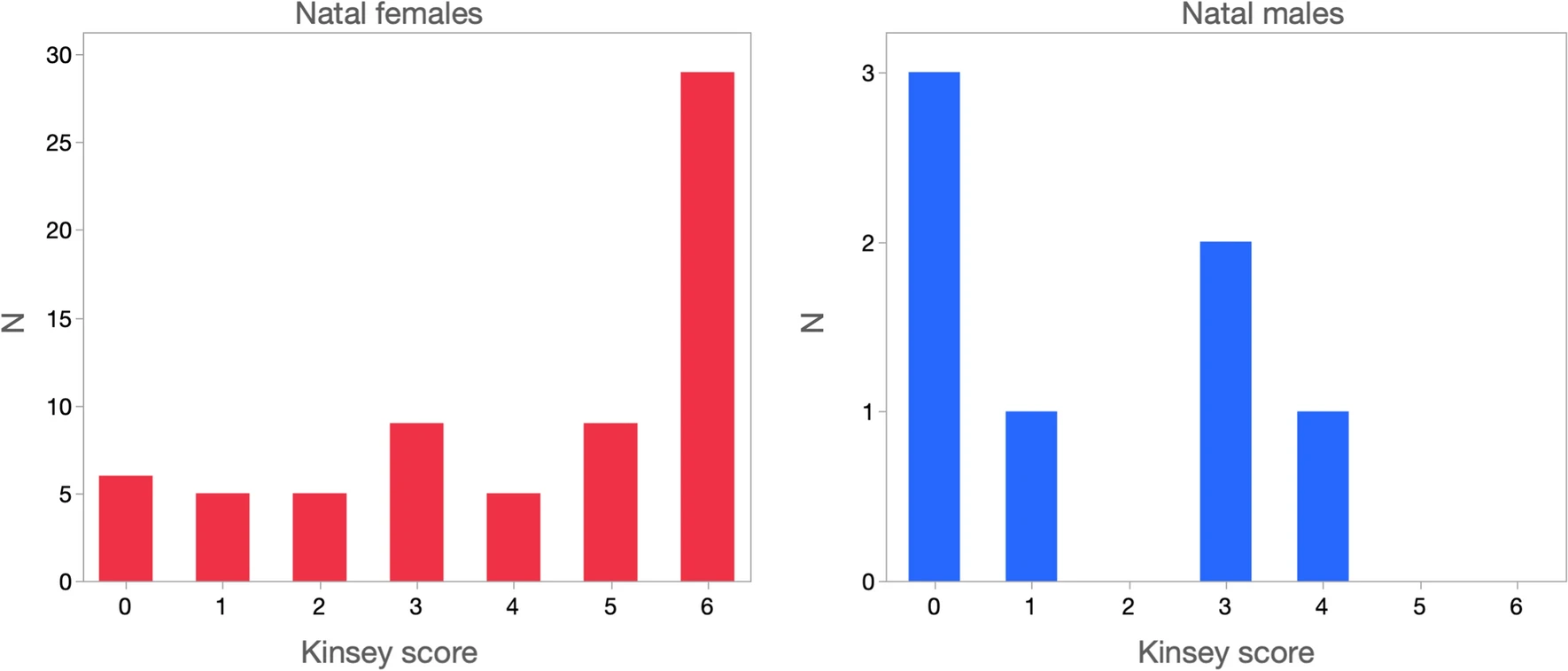
The next bit of data is the huge natal sex disparity ratio found in which only seven (7) of the 78 individuals were natal males, and all of them were primarily heterosexual or (self-reported) bisexual and 6 of that 7 reported sexual arousal to cross-dressing. This percentage (85%) is identical to that found among gynephilic transsexuals in a number of other studies. That is to say, that all seven were etiologically autogynephilic. This supports other observations that Male-To-Female (MTF) Homosexual Transsexuals (HSTS) simply do NOT detransition.
Interestingly, and likely much to Bailey’s chagrin, the data also showed that 15 of the 71 natal female subjects reported sexual arousal to wearing men’s clothing. Further, as expected by the theory that such autoandrophilia (AAP) would be found in heterosexual subjects, the correlation between sexual attraction to men was r=0.39. Bailey, even in this paper, tried to argue that such does not exist, yet here is more evidence that it does.
Interestingly, in support of the notion that most of these individuals, natal female, were not HSTS (Childhood Onset Gender Dysphoria), the authors report,
“Figure 1 presents the frequency distribution of summed scores across the eight items. The most common score (24.4%, N = 19) was 0, indicating endorsement of none of the items. Only 7.7% (N = 6) obtained the highest possible score, 8. The remainder of the sample was spread evenly across the scale, with points of rarity at 1 (only one item endorsed) and 7 (all but one item endorsed). Because we did not ask about two diagnostic requirements (duration of at least six months and distress or impairment), at most 16.7% (N = 13) of participants could have met diagnosis of DSM-5 Gender Dysphoria in Childhood (endorsement of at least six of eight items).”

Most of them, given that around half were mostly gynephilic girls, presented as tomboys, preferring boyish toys, etc. But a goodly number presented as gender typical in all respects. This is very much in keeping with the complaint of HSTS transmen, that many of these individuals weren’t the least bit gender atypical nor even very gender dysphoric in real life, how ever much they may have claimed to have been before they “detransed”. (Recall that 25 of them never “transitioned” in the first place.)
The study also found that the majority of these individuals come from very liberal family and community backgrounds, which would support their assertions that they were “trans”.
Overall, this study fully supports all of the conclusions that I and others have made regarding detransioners: 1) That among MTFs, it is universally autogynephiles (AGPs). 2) Among FtMs, it is largely “TransTrenders” from liberal families. 3) That these individuals have a high comorbid mental health diagnoses rate prior to claiming to be “trans”. 4) That in spite of these findings, such actual regret and detrans is rare.
Further Reading:
Where Are All These “Detransitioners” Coming From?
Transsexual Post-Op Regret Is Rare
Autoandrophilia in Androphilic FTM Transsexuals
Natal Females Falsely Claiming to be “Trans”
Reference:
Littman, L., O’Malley, S., Kerschner, H. et al. Detransition and Desistance Among Previously Trans-Identified Young Adults. Arch Sex Behav 53, 57–76 (2024). https://doi.org/10.1007/s10508-023-02716-1
Comments Off on Insights Gleaned From “Detrans” People
Boys Don’t Cry

Crying is a fraught subject; so many possible cultural myths and stereotypes to wade through to get to the real truth about why we cry and whether there really is a difference between men and women with respect to crying. On the one hand, we have social constructionists claiming any differences is purely because all gender differences are socially constructed, that “male socialization” tells boys that “boys don’t cry”. On the other hand, we have cross-cultural studies that show while the acceptability of public crying vary, the trend exists even there that women still cry more often and for longer when they do cry. But in no culture have they found that men never cry.
The causes of crying seem to be different as well. Attend any wedding and one can see a number of women crying tears of emotional joy, but rarely will you see a man doing so. Women even choose to read and watch stories that induce such. I know I do. I distinctly recall crying one afternoon as a teenager from the sad ending of a story about a boy, who in the dies by accident because his curiosity about how things work led him to get too close to moving machinery. I still cry at the end of my favorite Rom-Coms, like You’ve Got Mail. The morning after our parents announced that they were getting divorced, I couldn’t eat breakfast for the uncontrollable weeping, which my siblings and mother found embarrassing and unseemly. When I was kicked out of the house by mother at 18, I cried and cried. When I was evicted from my first rented room a few months later, I spent the night crying. When I was dealing with tough issues about adopting Liz, and her emotional troubles, I cried many a night. I cried at work when I was fired for being transsexual, from a job which I had invested four years of life and had risen to a respected position. I can’t tell you how many times I cried over a break-up with a boyfriend. The most intense crying bout I have had was when I took a phone call while in the clean room, standing next to the wall, being told that my beloved grandmother had passed. The other women in the clean room (pink collar job) had to lead me to a chair as I was totally blind from the tears and sobs.
I only knew of three times that my father cried, once when he was dealing with severe pain from illness. (In spite of that, he lived to 92), then next when he told me one night that his wife, my mother, had asked for a divorce. the third time I could hear him crying on the phone the night he called me when I was in the hospital, having had “sex change” surgery that morning, saying that I had “ruined” my life, that I “could never go back”.
Strangely, I have NO memories of my mother crying, ever. And she absolutely despised it when I did, often making disparaging remarks, saying in a deeply reproving tone, “You heart is one your sleeve”.
So, casting personal anecdotes aside, we turn to science and data to learn more about why we cry.
First, one learns that human tears contain prolactin, the hormone that induces lactation. Women, especially those in their fertile years, produce far more prolactin then men. There seems to be a connection between prolactin levels and the amount of tears produced. This might explain some of the difference between men and women in the length of time spent crying once a bout had been induced.
The second finding is from a very recent paper showing that mammalian female tears, including humans, reduces male aggression, from the abstract:
Rodent tears contain social chemosignals with diverse effects, including blocking male aggression. Human tears also contain a chemosignal that lowers male testosterone, but its behavioral significance was unclear. Because reduced testosterone is associated with reduced aggression, we tested the hypothesis that human tears act like rodent tears to block male aggression. Using a standard behavioral paradigm, we found that sniffing emotional tears with no odor percept reduced human male aggression by 43.7%. To probe the peripheral brain substrates of this effect, we applied tears to 62 human olfactory receptors in vitro. We identified 4 receptors that responded in a dose-dependent manner to this stimulus. Finally, to probe the central brain substrates of this effect, we repeated the experiment concurrent with functional brain imaging. We found that sniffing tears increased functional connectivity between the neural substrates of olfaction and aggression, reducing overall levels of neural activity in the latter. Taken together, our results imply that like in rodents, a human tear–bound chemosignal lowers male aggression, a mechanism that likely relies on the structural and functional overlap in the brain substrates of olfaction and aggression. We suggest that tears are a mammalian-wide mechanism that provides a chemical blanket protecting against aggression.
A chemical signal in human female tears lowers aggression in males.
.
The key is that the male has to smell the tears running down the females face or wiped onto their paws, etc. One can imagine in humans, the man has to have some close contact in order to smell this chemosignal. I have to wonder what would happen if a man who is attacking another he perceives as male and smells this signal. Will it reduce his aggression? Would it help protect feminine males such as homosexuals or homosexual transsexuals? Or would it backfire and make them more aggressive to the point of beating and murdering them?
The next question we need to ask, is this difference in crying between men and women based upon an organizational or activational effect of hormones. Does Hormone Replacement Therapy (HRT) for transsexuals cause changes in the number or intensity of crying? There have been many anecdotal reports that it does, but frankly, these are suspect due to the differences between reports from autogynephiles (AGP) and homosexual transsexuals (HSTS), the latter of which report no changes in weepiness upon starting HRT. (I certainly did NOT notice any such change, having always exhibited high levels of crying before HRT.) The other anecdotal evidence comes from straight men who are treated for prostate cancer in which it is claimed that the reduction in testosterone increases emotional labiality, including crying. However, when I tracked down the data, they were all from men who were extremely ill. As we know, pain, illness, and loss of sexual function in men can be very stressful, leading to depression, sadness and the need to express such through tears. Thus, the confound casts the anecdotal evidence in doubt.
Further Reading:
This is your brain; This is your brain on hormones
Further External Reading:
https://www.thecut.com/2015/01/why-do-women-cry-more-than-men.html
References:
Agron S, de March CA, Weissgross R, Mishor E, Gorodisky L, Weiss T, et al. (2023) A chemical signal in human female tears lowers aggression in males. PLoS Biol 21(12): e3002442. https://doi.org/10.1371/journal.pbio.3002442
Comments Off on Boys Don’t Cry
The Catholic Church’s War On Women and LGBT Families
Today, the Poop in Rome (not a typo), has fired yet another salvo against women’s reproductive choice and control of her own body, and at the very same time, attacked gay male and androphilic MTF transsexuals families, by calling for a universal ban on surrogacy.
The church has long insisted that any form of birth control, and especially abortion, is verboten, not just for their own adherents, but for all women. The goal was clear, control of women’s bodies and their sexuality. Indeed to “punish” women if they have sex such that they will likely become pregnant. For women having heterosexual sex outside of marriage, this would lead to an unwanted pregnancy that would shame them in their communities and force them, to enter “homes”, institutions, for unwed mothers such that the church could then steal their newborn babies and give them to infertile heterosexual married, “good Catholic” families.
Then, along came more readily available birth control methods and the “sexual revolution” freeing women from the worry of an unwanted pregnancy. Along with that freedom came the demand from LGBT for equal rights and in the past two decades, marriage equality.
Surrogacy had been around for centuries, in which families would help out an infertile female relative by volunteering to carry that relative’s husband’s baby and allow that relative to raise that child as her own. So called “commercial” surrogacy has been around for decades such that laws and customs have grown up around it to address various concerns. As long as it was about helping infertile heterosexual married couples, the Church had nothing to say about it, treating it much like they had their own practice of stealing infants from unwed mothers.
But with the growing social acceptance and legal recognition of gay and lesbian couples, something that that the Church fought against, the availability of both in family / altruistic surrogacy and “commercial” surrogacy has now led to gay male couples and androphilic MTF transsexuals married to straight men availing themselves of this practice, much to the dismay and disgust of the ‘phobic Xtians and now the Poop himself, in a despicable speech.
This, like the Church’s push against reproductive choice, birth control and abortion, we must fight against this latest assault on women’s rights to bodily autonomy to be a surrogate and the right of gay men and transsexuals to such.
Further Reading:
Further External Reading:
Comments Off on The Catholic Church’s War On Women and LGBT Families

Comments Off on Exploring The Science of Transsexuality