Are Drag Queens and Homosexual Transsexuals In The Same Spectrum?
Back in the ’90s, when I was teaching about our history, a gay man boldly asserted that since he had been an amateur drag queen that he and I were similar. I chafed at the suggestion that his dressing up in a costume for a few hours a week for a year was anything akin to my living full time as a woman since I was a teenager.
But recent online squabbling about the erotic role of “homosexual transsexuals”; HSTS being obligate bottoms and “avoidant” vs. a small minority claiming that HSTS can also be tops has me asking the question, “Are drag queen and HSTS in the same taxon / spectrum?”
There are those that would say, of course they are, because they are both “homosexual”. But given recent studies that very strongly show that there are two different discernable subpopulations of androphilic males, with different etiologies, biodemographics, behaviors, and even biomarkers, is this true?
Before continuing, if you haven’t already, please read the following essays so that the rest of this essay will make sense (Yes, I know that’s a lot of reading homework):
HSTS are more likely to exhibit the Fraternal Birth Order Effect (FBOE)
FBOE is caused by maternal immune system and does effect first born males
FBOE is associated with being shorter than average (on average)
Common Correlations between HSTS and Bottom Gay Men
2D:4D Digit ratio supports the two type taxonomy
2D:4D Digit ratio difference between Top and Bottom Gay Men
After reading this, it should be clear that there is significant evidence that at least the majority of HSTS come from the “bottom” subpopulation of androphilic males, which is very likely etiologically (perhaps even taxonicly?) distinct from “tops”. But what of Drag Queens?
Here, there is less published studies from which to marshal solid data and evidence. We are left groping for data from anecdotes and stereotypes, the worst and lowest form of evidence, if evidence it can be called. Yet, we can sometimes glean some indications.
One of the problems with delving into this question is that historically, HSTS often took jobs as “female impersonators”, performing on stage in a similar fashion as drag queens. Even today, some putatively HSTS use drag shows and contests (e.g. Ru Paul’s “Drag Race”) as a launching pad for careers as entertainers. But a key difference is that they choose to transition full time and upon casual observation, appear to fit stereotypical HSTS profiles while those that don’t fit a very different stereotypical profile.
So lets talk about the stereotypical drag queen. He is significantly taller than average for a man. He is also a “top”. Some even suggest that they are “catty” or “bitchy” (more so than an average gay man). Although perhaps this last is merely apocryphal.
Consider the ur drag queen, Ru Paul himself, who stands 6’4″ tall. This may be an outlier but examine the contestants of his show, many of whom are also well above male average (for the US, that average is 5’10”). Some are shorter, at about 5’7″ to be sure. So, it is true that drag queens tend to be taller than average? We simply don’t have any good statistical data.
The next question is whether draq queens are tops or bottoms. Here we have a very powerful community stereotype that the typical drag queen is most definitely a top. From an online article posted by a gay man attempting to dispel “myths” about drag queens,
5. All drag queens are tops.
OK, I’m hoping everyone reading this knows what I mean by “top,” so I’m not going to explain. Anyway, I never knew about this myth until after getting involved in the drag community, and it definitely is not true. I know several drag queens who are not tops. That’s all I’m going to say on this topic!
Ummm.. so he knows “several” who aren’t. That is another way of saying that most are in fact tops in his experience. Stereotype confirmed.
Getting back to the topic of whether HSTS and drag queens are in the same subpopulation. What scanty evidence we have says, no; No they aren’t. But what of those who claim to be HSTS and to be tops?
A few years ago, when I posted an essay on 2D:4D ratio showing that HSTS have very high ratios, an androphilic pre-op/non-op MTF transwoman wrote wrote to me saying it couldn’t be true because her ratio was very low, her ring finger being much longer than her index finger. It did not surprise me to later learn that, far from being “avoidant”, she was a proud top.
I’m reminded of something that I heard on occasion in the late 1970s (before the HIV/AIDS epidemic reduced their numbers), when HSTS gathered at various late night cafes and diners (some sex workers on a break, others just coming for the company), speaking of someone I wasn’t familiar with, “She’s not a transie… she’s just a drag queen!” At the time, I put it down to being a bit catty perhaps. But then again, perhaps it had a grain of truth. That some folk that better fit the category of “drag queen”, top, more masculine, taller, older when they began their career of dressing as women to enter the company of HSTS on the street… that perhaps even today, some “drag queens” seek to live as “trans”, get breast implants, perhaps facial surgeries (FFS), etc. and of course top men who seek out “girl dick”, for fun and profit. And perhaps some insist that they are HSTS, because they are in truth ‘homosexual’.
Further External Reading:
https://www.huffpost.com/entry/10-myths-about-drag-queens_b_2979249
Further Reading:
Contrapoints for the Wynn
Even as Natalie Wynn (AKA “Contrapoints”) attempted, and failed, to “debunk” autogynephilia as a phenomenon and etiology, she elucidated the two taxons “homosexual” vs. “autogynephilic” transwomen perfectly. I don’t know who captured her descriptions of the two and put them into this wonderful photo meme, but thank you for doing it.

I want to examine each of the items and link to my essays covering the science that supports them. Oh, and as the meme asks, I will use it to “sort” myself according to them.
The first item is a separation on sexual orientation. This one is axiomatic in the Two Type Taxonomy. But is sometimes problematic in that many MTF transsexuals will falsely claim to be androphilic due to autogynephilic pseudo-androphilia and social desirability bias. But, we can sort based on sexual history using various clues like legal marriages to women and having sired children. Key questions to ask is if the individual has had sexual intercourse with a female person vs. having sex, especially as a “bottom”, with men, pre-op. Cluster A are very unlikely to have ever had Penis In Vagina (PIV) sexual intercourse with a woman. And Cluster B are very unlikely to have NOT (save for very young, pre-sexual debut and “assexual” behaving individuals) to have had PIV sex.
Essay on MTF transsexuals misrepresenting their sexual orientation.
Personal history:
I can say with absolute honesty that I NEVER had PIV intercourse with a female, nor did my ahem… enter any other orifice, period. (And had plenty of offers in high school and college years.) Yet, I was very sexually active with men, as an obligate “bottom” (and “avoidant”) pre-op. My sexual debut was at age 18 w/ a 25 y/o buff man. I then continued to date and have sex with a number of men, both while pre and post op. Jeff Elliott, my husband and I will be celebrating our 24th wedding anniversary in a few weeks.
So, one point in the Cluster A category.
Second item is about age of transition. Multiple clinical studies have shown that there is a clear bimodal distribution of age for transition that is highly correlated with sexual orientation. Half of androphilic transwomen socially transition and begin HRT before age 20, and almost never after age 25. While for Cluster B, the data shows that the median is around 35 and the average 40+.

Essay on study showing early transition for androphilic transwomen.
Essay on study showing bimodel onset of gender dysphoria and transition.
Personal history:
Starting in Jr. High, I wore girl’s style cut-off (“hot pants”) and girls shoes (moccasin flats). I began more overt social transition while still in high school, first beginning presenting as a girl with friends at their homes at age 15, openly in public, shopping, hanging out, etc. by age 17. Full time right after graduation the same week I turned 18. (I had to present as a “boy” at school since my two brothers were also students there and my ‘rents were VERY disapproving, etc.) I started HRT at age 18 as soon as I was legally of age to consent to my own medical care.
So, two points for Cluster A category.
The third item is about gender atypicality as a child. Clinicians have long noted that the two types are very different on this score. However, one can’t trust self-report as Cluster B types tend to “shade” their personal memories. One really should get that information from older family members (parents, grandparents, etc.)
Essay w/ data on self-report of gender atypicality.
Personal history:
Let’s review what my mother told Dr. Fisk at the Stanford Gender Dysphoria Clinic about my childhood behavior in ’75 (when I was 17): “I have known for years that he wanted to be a girl. But I thought that was [morally] wrong. He was very different than his brothers. All their friends were boys. His were always girls,” naming several of my friends over the years, starting with my pre-school friends, but couldn’t remember my friend who had been my only guest on my tenth birthday. “Marian,” I interjected for the only time during the whole interview. “He was always very prissy. He would walk clear around even the shallowest puddles. When he was little, I would put him in clean clothes on Monday and on Friday they would still be clean.” She confirmed that I had been sent to a therapist about my behavior when I was ten years old… and again when I was 15/16.
So, three points for Cluster A.
The forth item is about being bullied vs. being a bully. I have no solid data regarding this, but many clinicians have written about how classic / “true” transsexuals were bullied as children. I’ve seen little to no data on Cluster B types being the bullies, though anecdotal stories from clinicians talk about how many of their patients express misogynistic / homophobic attitudes. Goodness knows, some of them are serious bullies as adults post-transition.
Essay on clinical description of misogynistic attitudes in Cluster B clients.
Personal history:
One of the worse beatings I suffered was when I was 14 years old, when two older boys, who laid in wait along my path through a dark orchard one winter evening, just a block from my home, first taunted me, then beat, knocked me to the ground, and proceeded to kick me viciously, all the while yelling homophobic slurs. Their exact words included,
“FAGGOT!”
“PANSY!”
“PANTYWAIST!”
“YOU THINK YOU’RE A GIRL?”
“YOU MAKE ME SICK!”.
Our family moved from a solid middle class neighborhood to an upper middle class one nearby and we transferred to another high school nearby, Los Altos High, with a zero tolerance policy toward bullying. I was grateful for that policy, because it mattered. One day, during my Senior year (well after I had come out), a boy I didn’t even know (so this wasn’t personal) approached me during lunch while I sat with several friends on the Senior Lawn, began kicking me, yelling,
“GET UP FAGGOT AND FIGHT!”
I looked up at him and told him, “You are barking up the wrong tree, I won’t fight you.” Two of my female friends put themselves between him and me when he resumed kicking me.
So, four points for Cluster A.
The fifth point is Cluster A being confused for a girl while pre-transition, while Cluster B being thought of as an older man. This one is more anecdotal perhaps, but their IS data on differential passability which may relate AND I do have a couple anecdotes about my adopted daughter insisting that a post-op “Cluster B” was a man, but saw a pre-transition Cluster A teenager (19 y/o) as a girl even though she was wearing boy’s clothing.
Essay on differential passing ability.
Essay on w/ anedotes about a teen passing as girl pre-transition
Personal history: This one I can’t provide data other then I was successfully passing as a girl in public several years before starting HRT. It might have happened other occasions and I hadn’t noticed… save for the time I was 14, my first week of high school, when one boy asked another, “Is that a boy or a girl?” and the other just shrugged in indecision. I can say that NO ONE ever thought I was an older man. People often thought I was much younger than my actual age (until I transitioned full time).
Is that still four points or five for Cluster A? Definitely NOT Cluster B.
The sixth item is about how tall the two clusters are. Here we have many anecdotes from clinicians mentioning this difference, but only two studies testing it, which had conflicting results. One clearly showed that Cluster A was shorter (and lighter boned, which is item #13).
Essay on height and build differences.
Given that we also know that Cluster A types (HSTS) are “bottoms” and that as a class, bottoms are the ones who exhibit the Fraternal Birth Order Effect (FBOE), we have data that shows that there is a correlaiton between FBOE and being shorter than average.
Why Cluster A (HSTS) are short
Personal stats: I am 5’7″ and the day I turned 18 years old I weighed 130 pounds. The day I had SRS at age 23, I weighed in at 125 pounds. On my wedding day, I weighed 135 pounds.
So, another couple points for Cluster A.

The next item is digit ratio. This is referring to the 2D:4D ratio, the relative length of the index vs. ring finger. I have quite a few essays talking about this metric. This does seem to be true that Cluster A has a higher 2D:4D ratio due to feminizing hormones prenatally.
Essay on 2D:4D ratio supporting the two type taxonomy.

Personal stats: I love this one. Here is a photo of my hand. My 2D:4D ratio is “off the chart” high at 1.06 !
Chalk up another point for Cluster A!
The next two items are delayed puberty and weaker puberty. These are more anecdotal in that only recently have scientists been directly monitoring transsexual youths. But anecdotally, we do have some evidence for this in that Cluster A types tended to be older for each Tanner milestone and that they have less body hair and smaller genitalia. The same regarding Cluster B in reverse. I don’t have any essays or know of any good papers on the subject. But we’ve all seen it on each other.
Personal history: When I turned 18 and began HRT, I had zero facial hair, no “body hair”, my pubic and underarm hair was sparse, light, and in the female pattern (downward triangle). When I had my initial consultation with Dr Biber for SRS, he remarked that I had extreme hypotrophy (lack of growth) of my genitals. I replied, “Yeah, its always been that way”.
Funny story: One day, in my early ’40s, while in the waiting room at the Sea Horse Medical Clinic (Dr. Joy Shaffer’s clinic for transfolk), a 30-something transwoman with recent electrolysis inflamed facial skin noted my smooth and clear face, asked me, “How many hours of electrolysis have you had?” Clearly she was hoping to gauge how many hours she would need to look like me. Feeling mischievous I feigned ignorance, “Electrolysis?”. “Yes, how many hours did it take you?” “Electrolysis?” Hearing this exchange, Dr. Shaffer, who had been my college roommate intervened, “That’s her primary growth.” “I hate you!” the transwoman said to me in mock jealousy.
Add another couple Cluster A points.
Next item is muscle mass. Save for the difference in passability (linked above) and the body build (linked above) I don’t have much actual studies on the topic. But, hey, we’ve all seen the difference!!!
Personal history: My parents, especially my mother, was always concerned with the lack of muscle mass. But even one of our high school P.E. coaches was in on the act (not the nice one who later rescued me from boy’s P.E. my senior year, after I came out). That *&^%$#@! forced me to take a body building class for P.E. F’ck that noise! I refused to do the work. I mean, there was no F’ing way I was going to push to look like a butch man!
Funny story: All of the kids got standardized “physical fitness” tests in high school. The same tests for both boys and girls, but the scoring was different on each item. Girls were not expected to do many (or even one) pull-up but were expected to be able to do more sit-ups than boys. I scored as “unfit”… on the boys scoring sheet. But as very fit on the girls, unable to do a single pull-up, but far more sit-ups than any of the boys, right in the norm for girls, across the board. It got me some teasing from those that hadn’t yet figured out that I was androphilic/transsexual.
Another point for Cluster A.
Then we come to “soft”. This is a reference to the amount of subcutaneous fat, typically a female trait. Sadly, I have zero data on this. But c’mon, many of us were known for being “soft” like that as teens. I was, no doubt about it. It was one of the reasons I could pass as a girl before HRT.
Funny story: When I was 14, I was wearing shorts (hot-pants really) one summer day, as I passed my brother and his buddies in the garage. One of the boys looked up and exclaimed, “You have girl’s legs!” and the other boys sniggeringly agreed. Yeah, my legs have always been my best feature.

Let’s add another point for Cluster A.
Finally, we have a reference to facial shape, rounder, smaller. Again, this feeds into the differential passibility study, etc. (linked above) It may sound catty, but we can usually tell if someone is Cluster A vs. B (that is to say, HSTS vs. AGP) just from a photograph of their face. Facial Feminization Surgery has shifted this somewhat… but if one sees a “before” HRT and FFS surgery facial photo, there is no question that Cluster B’s look like masculine men.
The photo shown here is my Jr. College ID taken in the summer of ’75 at age 18. This photo was taken several weeks BEFORE I started HRT. That does NOT look like a butch face. Yes, I started living full time as a woman before HRT.
Add another Cluster A point.

Add it all up… add up all the points for the win… As they suggest, I fit the Cluster A very, very well.
Further Reading:
Magazine style quiz to access if one is HSTS vs. AGP
Comments Off on Contrapoints for the Wynn
One’s Job or Education Do NOT Define Either HSTS Nor AGP Transwomen
— Just as one’s job or education do NOT define men nor women.
For over a decade, I’ve been writing on the Science of Changing Sex, explaining how the science supports the Two Type Taxonomy. This after spending years researching, teaching, and writing about our history. (Trivia: many of the current texts on our history have borrowed rather heavily from that earlier work. No, I’m not upset by that, but pleased it has become so well known.) That after having worked as an early transsexual rights activist, including joining with several other transsexuals to form the ACLU Transsexual Rights Committee in 1980. This early work almost certainly set the stage for later activists to join in that work.) Sadly, while there has been progress in understanding the nature of the Two Type Taxonomy, there is a continuing denialist opposition to it. That opposition has not restricted itself to respectful scientific arguments, but often descends into personal attacks, calumny, and character assassination.
Please Read “What The Next Wave of Transgender Activists Need To Know”
One of the silliest of these is based on mistaken sexist stereotypes about the differences between the two types, sadly started by several of the top sexologists that researched the taxonomy and support further research and education, to wit, that Autogynephilic (AGP) transwomen are very likely to be “geeky” and become scientists, engineers, and technologists while Homosexual (HSTS) transwomen are not. This is based on the totally erroneous idea that straight men are more interested in these careers than either women or gay men, by nature. The other false stereotype is that HSTS are too stupid to have such careers, having lower IQ than average. This too was started by an offhand personal obsersation by a sexologist.
Please Read “Stereotypes Are Dangerous” and “The Right Stuff”
The reality is that women are just as likely to be interested in such educations and careers as men, when given the chance and not discouraged from doing so. And HSTS show the same average IQ as the general population, though very rare, there are HSTS with very high IQs.
Please Read “Tech Bros and Silicon Valley’s Misogyny Problem”

From the graph, we can see how women, when the sexist limits on their enrollment in the physical sciences, legal, and medical fields were reduced, the percentage of women seeking degrees in those fields climbed and now has reached near parity with men. Computer Science is the only field where the enrollment initially climbed, then fell off. It was NOT that women didn’t like the field. It was and remains a problem of a toxic culture in computer programming where immature, misogynistic, young men make studying and working in the field a hostile environment for women.
Women have long wanted to be scientists and technologists. Consider these women: Ada Lovelace who worked with Babbage on the concepts of computer programming before computers existed; Maria Sklowdowska Curie who was awarded, not one, but two Nobel prizes in physics and chemistry; her daughter Irène Joliet-Curie who also won a Nobel prize in chemistry; Lise Meitner, who should have won the Nobel Prize for the discovery of atomic fission that led to nuclear power. The list is long. Although these are extraordinary women for their accomplishments, they are not unusual for being interested in science.
I would argue that gay men are also just as likely to be interested in these fields, though we don’t have as much documentation to prove it. But consider Alan Turing, one of the most celebrated mathematicians and computer pioneers of the 20th Century, was gay. Today, we have Tim Cook, CEO of Apple, Inc., one of the most successful Silicon Valley companies. The most amazingly brilliant technologist who ever reported to me was an undergraduate summer intern from MIT in the early ’80s. When he later came out, he asked me if I knew he was gay before. “I knew the day I hired you!”. He later earned a Ph.D., published a textbook on robotics, and became a Silicon Valley executive.
The stereotype of autogynephilic transwomen being geeky also fails to hold water when we look at them and note how many have careers that are not at all “geeky”, but are stereotypically male/masculine coded like law enforcement, military, construction, transportation, etc. Then there are the number who are living in poverty and squalor because they have no marketable skills acceptable to (accepting of) women post-transition.
Thus, women and gay men like and pursue education and careers in the physical sciences and technology just as much as straight men. But straight men will avoid fields that are coded as “women’s work” or feminine/”gay”. Autogynephilic transwomen notoriously have the same aversion pre-transition. So, while we can NOT use pursuing an education in the sciences or working in technology as a useful marker for autogynephilia, nor as exclusionary of being homosexual (transsexual or not); we can use female coded careers and jobs, especially those pursued before transition, as likely exclusionary of being autogynephilic and also increasing the odds that such an individual is homosexual (transsexual or not).
Back to the issue of what does define and differentiate the two types of transwomen. Very simply, their sexuality. One is gynephilic and autogynephilic, the other is androphilic (homosexual w/ respect to their natal sex). Nothing else defines the two types.
However, there are indicia that highly correlate with the two types. In my years of examining the science literature I have found seventeen independent lines of evidence that correlate and supports the two type taxonomy. None of them are educational / career interests. Some of these correlates can only be used at the population level, but several can be used at the individual level: gender atypical behavior as a pre-adolescent, age of onset of gender dysphoria, age of social transition, and of course, definitionally, sexual history (showing actual sexual orientation).
Please Read the first few entries in the “FAQ on the Science of Changing Sex”
The Personal Is Political
Back to the problem of the denialism and of the calumnious attacks, specifically, those attacks on me. In an ironically revealing, one might even say, self-own, they simultaneously claim that there is no two type taxonomy and nearly in the same breath tell me to shut up because I must be AGP as well because of my interest in the sciences and my long career in Silicon Valley! But as I showed above, that does NOT define nor differentiate the two types. But if one examines my bio, one can find all the indicia needed to determine which etiological type I fall into.
Please Read “About”
Consider this section to be an expansion of my bio, focused on those indicia. As I said in my bio, the only honorable defense against lies is the truth.
My mother, during an interview with Dr. Fisk at the Stanford Gender Dysphoria Clinic, complained bitterly about my early gender atypical behavior, under the false impression that he would be attempting to “cure” me. I was but 17 years old at the time.
“I have known for years that he wanted to be a girl. But I thought that was [morally] wrong. He was very different than his brothers. All their friends were boys. His were always girls,” naming several of my friends over the years, starting with those when I was five and six years old, but couldn’t remember my friend who had been my only guest on my tenth birthday. “Marian,” I interjected for the only time during the whole interview. “He was always very prissy. He would walk clear around even the shallowest puddles. When he was little, I would put him in clean clothes on Monday and on Friday they would still be clean.” She confirmed that I had been sent to a therapist about my behavior when I was ten years old and again when I was 15/16.
When I was nine years old, at the end of 4th grade, our elementary school was planning one of those embarrassing shows where students perform for their parents and friends. I’m sure you know the type I’m talking about. I was cast for a part but when told the details of the part, I had a total emotional melt-down, tears, loud drama, refusing to take a male role. It set off a chain of interviews and behind the scene discussions with my parents that I only learned about years later. The next school year, I was required, by the school district psychologist, to be sent to a very special therapist some miles from our home, to “play” and talk with Dr. Peters every Friday afternoon. Interesting thing about the playroom. It had only boy’s toys, which held zero interest for me. Sometimes, we played chess, but otherwise, we only talked. Why?
Please Read, “Shameful History of Reparative Therapy of Transsexual and Gay Children”
I’ve already disclosed a few details about how in Jr. High, I spent my time at the library reading about girl’s fashion, make-up, etc. I also practiced putting on make-up, borrowing my mother’s, given that we had the same coloring, etc. I was always careful to put everything back exactly as I found it and to wash my face carefully, but she knew I was doing it. She just couldn’t catch me at it.
One of the stories my mother would tell other mothers, often in my presence to try to embarrass me, was about the day she was sitting out on the lawn pulling weeds when she saw me at a distance walking home from school. When I saw her, I discretely adjusted the stack of books I was carrying (female style, books against my chest, if you must know), sadly not discretely enough. She would tell her listeners that she was convinced that I must be bringing home and attempting to hide, pornography, so she later searched my room. What she found instead was a book on manners and etiquette for teenagers, mostly for girls.
When I was fourteen, my freshman year in high school, Debra asked me to the Sadie Hawkins dance. I loved dancing and she was one of my friends so I agreed. A couple weeks after the dance, she invited me over to her house. Her mother wasn’t home as I had expected her to be. Debra went into her bedroom and changed out of school clothes and into a very revealing, slinky dress. She literally draped herself across me as I sat on the front room couch. Disturbed, I pushed her off of me and jumped up off the couch. She tried to cajole me into rejoining her on the couch but I refused, as I paced the floor. She gave up and changed back into more modest jeans and top. The next day, as school ended, she again invited me over to her house, but I turned her down. Debra broke into tears and ran away. We never spoke again.
During the next summer, just after I turned 15, I took square dancing classes with one of my female friends. I paid special attention to the girl’s part, intending to attend square dances as a girl, and dance with the cute boys. My friend supported this plan and lent me one of her square dancing outfits. My mother discovered the plot and forbid me to attend any more lessons and forced the return of the outfit.
Another girl, who was in the square dancing crowd freaked out and cut me off when I came out to her. Thank goodness we didn’t go to the same school. But I hated losing friends.
We moved to a new house in a nearby suburb a couple months after that and I transferred to the local high school. I joined up with a crowd of kids that included a boy, Greg, I had known in Jr. High. He now lived with his mother and new stepdad, while his brother Jeff (Not my husband Jeff) lived with his dad and attended my old high school. Thus, my circle of friends doubled as I kept in touch and occasionally met with my old friends. One of those old friends, Dennis, would meet me half-way, at Cassie’s house. Dennis was very comfortable being affection with me, often letting me massage his back or just sitting close. One day, at Cassie’s, the two of them started making out hot and heavy right in front of me. The green eyed monster joined us and took over. I stormed out, slamming the door as hard as I could. For the next week, Dennis tried calling me several times a day. I just hung up on him as soon as I heard his voice. After a week, Cassie called. I wasn’t mad at her. She could make out with any boy she wanted as far as I was concerned. Cassie said to me, “You have punished him enough.”
So, with that we agreed that I would go to Cassie’s and talk to Dennis, to patch things up. But I had a plan. Cassie agreed to let me come early and borrow her clothes. She was two inches taller and a bit bigger, but her dress size was close enough to mine. I met Dennis wearing a cute blouse with a jumper dress over it, panty-hose and nice shoes. Dennis and I talked pleasantly, never once making any reference to how I was dressed. I was trying to let him see that I was attracted to him, etc. He didn’t reject me, but wasn’t going to be dating me either. Oh well… I tried. Skipping forward three years for just a moment. Dennis visited me right around graduation. During a walk around the block, away from other’s ears, he asked, “You going for that sex change?” I answered simply, “Yes.” Upon which he said, “Good luck.” and hugged me.
That same year, aged 15, my mother decided it was time she dealt with me and my “homosexuality”. She first took me to our family doctor for a physical and a consult about it. There didn’t seem to be anything physically wrong, save that I was “underdeveloped” (and stayed that way, thank the Blessed Goddess… At 15 I was perhaps at Tanner stage 3, I never reached stage 5). He recommended a therapist, Dr. Kanski, who I had to see once a week to “talk about my problem”. I would talk very pleasantly about almost any subject, but my sexual orientation and gender dysphoria / identity. Dr. Kanski later told my mother that I was “uncooperative”.
Around this time Jeff introduced me to his best friend Kevin. I had a huge crush on him for the rest of my time in high school. Jeff and Kevin occasionally came over to our house. My mother would notice that I got excited each time they did this, but thought it was Jeff that I had a crush on.
Later that year, as I was helping Cassie with her homework (I was often asked to help others and gladly did so), she reached under the table and grabbed my genitalia, saying in coquettish voice, “My mother won’t be home for hours.” I was horrified! I pulled her hand away from me and pretended nothing had happened. She started to slide her hand to my crotch again but I grabbed it and held it tight against her leg, while continuing to explain the homework problem. I was hurt and angry. She knew about my transsexuality. Why would she should do this?
The summer, just after I turned 17, I got a job as a full-time nanny taking care of two boys, ages ten, and four. Their mom later wrote a letter of introduction and recommendation using my new name and gender. The family also gave me some of her older, but stylishly appropriate for a teenager, clothes that would fit me.
Our house was next door to our community pool. We often had friends over for a swim, including Cassie and Barby, among others. One day, I picked up Barby from her house in our family’s spare car to go for a swim. She was wearing a skimpy bikini and nothing else. As we were going down the street, she grabbed my hand and pulled my hand to her crotch. (You just know that a straight boy would have loved it and also be having ‘trouble’ with his own.) I was never more grateful that I was driving a car with a manual transmission as I removed my hand back to the gear shift knob.
It was past time I came out to Barby.
My senior year I called our family doctor and asked for female hormones. His reply was, “You can do anything you want with your life, but I won’t be any part of it.” Soon after that I found a reference to the Stanford Gender Dysphoria Clinic. On the phone, they said I needed to have my parents make the appointments, etc. After some serious family drama, my Dad did. After the intake interviews with Dr. Fisk, I filled out their required paperwork at school, with friends looking over my shoulders, offering comments. Both of my parents tried to talk me out of transition.
Please Read “Cognitive Dissonance…”
A few months before graduation rolled around, I was out to all my close friends and word was getting around. Of course, the fact that I was often seen around town or at the mall with friends dressed as a girl helped that. But, I still had to present as a boy in class. I openly hung up my new wardrobe in my closet, earning silent glares of disapproval from my mother, but gave her a ‘I dare you’ look back. But after graduation, I was living full time as a girl.
At one point my father strongly suggested, “Have sex with a girl. I’m sure that will change you. What about one of your friends, Barby, or Cassie? Wouldn’t they do it to help you?” I replied angrily, “I’m sure they would. But that won’t change me and I DON’T want to have sex with them!”
I turned eighteen a week before graduation. My dad came over to wish me happy birthday and give me a present, the only one I got from anyone, a nice clock radio. I would need it as he also told me I was being evicted from my mother’s house and not allowed to move in with him.
I won’t go into details, that’s not anyone’s business; I dated several boys/young men from my circle of high school friends starting then and for the next few years. But one of my boyfriends, Jordan, from that time, later introduced me to his wife as his “first girlfriend”. Think about that, a straight man was proudly telling his wife that his first relationship was with a pre-op transwoman! Of the others, my mother had accused Jeff of being my lover. Wrong, he had rebuffed me… his brother Greg on the other hand… The one that really created family drama was Don, my brother’s best friend.
Barby complained, bitterly and unkindly, that I was “boy crazy”.

The relationship that lasted the longest was Bob. His mother was an engineer, president of the Silicon Valley chapter of the Society for Women Engineers. I was a welcome guest at their family dinners. She strongly encouraged me to study engineering. When he was away at Rensselaer, back east, we handwrote letters often and occasionally talked long distance on the phone. I learned from one of his housemates on the phone that when Bob was lonely, he would open the drawer where he kept my letters, just for the waft of my perfume I scented them with. When he was home… we dated on and off like that for several years. in the end though, he married my best friend Jan and raised two girls with her. But we remained friends. In fact, Bob attended my wedding to Jeff.
I remained friends with several female friends, most especially Jan and Robyne, occasionally sleeping over in their bedrooms. Think about that for a moment. Their families had known me for years…Robyne’s since Jr. High, do you think for one moment that they would let me be alone, in their teenaged daughter’s bedrooms over night, if they thought I might be interested or capable of having sex with them?
As to choice of careers. I love teaching and have been an instructor/tutor in several schools in several subjects, from teaching little kids swimming to teaching teens and adults flying. I started my career in Silicon Valley as a secretary / administrative assistant. I worked as an electronic assembler (a female coded job) and proceeded up the ranks of supervisor and management, all while earning a degree by examination after self-study. That’s not the career arc of a typical AGP.
So, remembering the definitions and indicia of sexual history & orientation, childhood gender atypicality (as reported by my mother), age of gender dysphoria onset, age of transition, etc. What type am I?
I have no doubt the AGPs in denial, haters, disappointed chasers, and TERF/GC folk will all still tell lies. But I know who and what I am.
Comments Off on One’s Job or Education Do NOT Define Either HSTS Nor AGP Transwomen
Gaming Transsexual Brain Sex Research
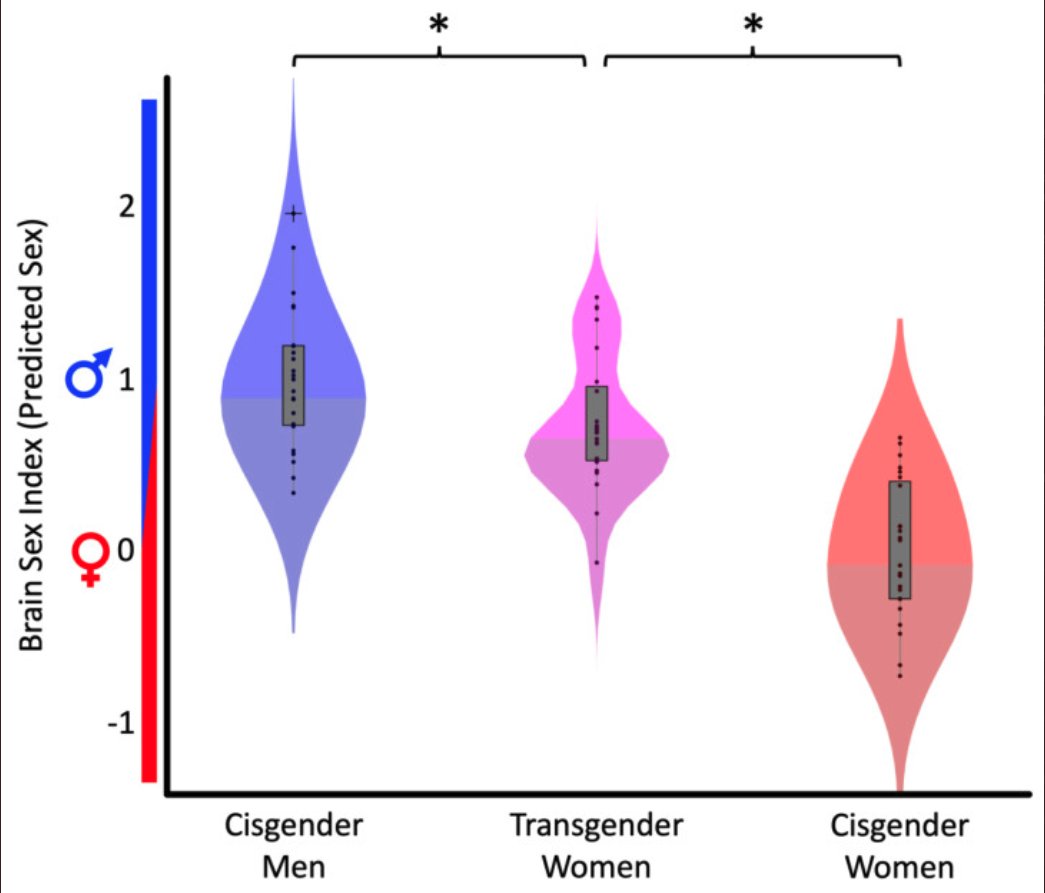
Another study done by Luders research group on MTF transsexual brains comparing them to control men and women shows a shift toward female brain phenotype. I’m sure this will be picked up by many transwomen and lauded as proof that they are “women inside”. Ummm… not quite so fast.
There are several issues to be addressed first. When I first learned of the study, I was dismayed that they had lumped the two types together. At this point in research history, this is inexcusable. In fact, the Luders group does know better, as they had cited Guillamon who specifically called out this mistake in past studies and recommended that they always be separated. Further, they didn’t look at sexual orientation in the control groups either.
This last may not have been that egregious, in that the control groups only included 24 subjects in each. The likelihood of including gay men and lesbians in such a small group is small and would not push or pull the results very far if there is a difference in brain phenotype from heterosexual subjects.
But lumping androphilic and non-androphilic transwomen together is not only a mistake, but given our current understanding based on previous brain sex research, which as Guillamon showed that only the androphilic type had female shifted phenotypes, guarantees that the whole will show a shift toward female phenotype for the whole subject group; which is likely the desired result of this current study, depending upon the ratio of androphilic to non-androphilic subjects, as the paper details,
Twenty-four transgender women (biological sex: male; perceived gender: female) were recruited through local community organizations and through professionals who offer services to the transgender community. To be included in this study, participants needed to self-identify as transgender women, report no history of hormone therapy, and declare the intention of undergoing estrogen replacement therapy. Moreover, participants were confirmed to be genetic males as defined by the presence of the SRY gene in their genome [53]. Six transgender women reported to be androphile (attracted to men) and 18 transgender women stated to be gynephile (attracted to women). The mean age of the transgender sample was 45.7 ± 13.8 years (range 23–72 years).
One might excuse this failure to examine the two types separately based upon the argument that the were already so few transsexual subjects and thus less likely to be statistically powered enough. But this is NOT a valid excuse. One could have done the analysis both ways. But I strongly suspect that would have defeated the ideological aim of the authors, as it would have demonstrated what those earlier studies also showed, that only the androphilic group had a female shifted phenotype. Instead, by lumping them together, one could give the false impression that MTF transsexuals as a whole show such a shift, if slight.
When I realized that they had lumped the two types together, I made a silent bet with myself, predicting that there would be a bimodal distribution, two “humps” in the data, indicative of two types, taxa, being lumped together. Sure enough, the violin plot of the transwomen shows exactly that!
Further Reading:
Essay on Guillamon Meta Analysis
References:
Kurth, F.; Gaser, C.; Sánchez, F.J.; Luders, E. “Brain Sex in Transgender Women Is Shifted towards Gender Identity” J. Clin. Med. 2022, 11, 1582. https://doi.org/10.3390/jcm11061582
Guillamon, A et al., “A Review of the Status of Brain Structure Research in Transsexualism” Arch Sex Behav (2016). doi:10.1007/s10508-016-0768-5
Comments Off on Gaming Transsexual Brain Sex Research
Brain Power…

“…I would while away the hours, confir’in with the flowers…. if I only had a brain…” — Scarecrow, in the Wizard of Oz musical film.
After years of trying to explain the differences between the two types and the statistical evidence for the two type taxonomy of MTF transwomen, I’m now posting what should be the final clincher; solid biomedical laboratory evidence, “proof” even.
Decades ago, as I was researching our collective history and science (the two often go hand in hand), I came across a reference to studies that showed that gay men had feminized brains while MTF transsexuals did not. SAY WHAT!?!?
Turns out, the study referenced made the false assumption that all MTF transsexuals are the same and had only included gynephilic older transitioners. Other studies, being aware of, and accounting for the differences between the two MTF transsexual types found something quite interesting, as for example, from the Dörner (1983) abstract:
“In male rats, androgen deficiency during a critical period of sexual brain differentiation was shown to give rise to a predominantly female-differentiated brain. Such animals displayed “homosexual behaviour”, i.e., they were sexually attracted preferentially to partners of the same sex. In addition, they exhibited a sex-specific evocability of a positive oestrogen feedback effect. A positive oestrogen feedback effect on LH secretion was also induced in homosexual transsexual men, in contrast to hetero- or bisexual transsexual men. Thus in homosexual transsexual men, an intravenous injection of 20 mg Presomen (Premarin) produced a significant decrease of serum LH levels followed by a significant increase above the initial LH values. In hetero- or bisexual transsexual men, by contrast, intravenous oestrogen administration, while producing a significant decrease of serum LH levels, was not followed by an increase above the initial LH values. A positive oestrogen feedback effect on LH secretion was also found in homosexual non-transsexual men, in contrast to heterosexual men. These findings suggest that transsexual as well as non-transsexual homosexual men possess a predominantly female-differentiated brain which may be based, at least in part, on androgen deficiency during sexual differentiation of the central nervous system. Homosexual transsexual men also showed an increased LH and FSH response to LH-RH as compared to hetero- or bisexual transsexual men.”
Note that non-exclusively-androphilic (“heterosexual or bisexual”) transwomen did NOT have the female like positive estrogen feedback effect on LH serum levels. Of course, according the Blanchard’s work, all “non-homosexual” MTF transsexuals should also be in the same taxon, so we would predict that so-called, asexual transsexuals should also show the lack of this positive feedback, and indeed, this too was found, as discribed in the Dörner’s (1976) earlier paper,
“In transsexual men with homosexual behaviour and intact testicular function, as well as in homosexual men with normal gender identity, following a negative oestrogen feedback effect a delayed positive oestrogen feedback action on LH secretion was evoked. By contrast, in transsexual men with hypo- or asexuality and intact testes or hypergonadotrophic hypo- or agonadism, as well as in heterosexual men with normal gender identity, a negative oestrogen feedback effect was not followed by a positive feedback action on LH release. In transsexual women with homosexual behaviour and oligo- and/or hypomenorrhoea, only a weak or at best moderate positive oestrogen feedback action on LH release was evocable, similarly as in castrated and oestrogen-primed heterosexual men. By contrast, in a transsexual woman with bisexual behaviour and eumenorrhoea, a strong positive oestrogen feedback action on LH secretion was evocable, as well as in heterosexual women with normal gender identity.”
Note that in this paper we see a mirror like difference between FtM “homosexual transsexuals” (gynephilic transmen) who respond more like heterosexual men and bisexual FtM transmen who respond more like heterosexual women. Thus, this data would lend support for there being a taxonic difference between exclusively gynephilic and non-exclusively gynephilic transmen, mirroring the taxonic difference between the two types of transwomen.
Conclusion:
These papers, detailing a specific, repeatable, laboratory based test that can differentiate the two types of transsexuals described by Blanchard, “Homosexual” and “Non-Homosexual”, offers both supporting evidence for the two type taxonomy but potentially also a way of independently sorting the two types in future studies. This difference is a classic medical biomarker for the two types. Should anyone one doubt the weight of statistical evidence, we can also point to the biomedical evidence via laboratory tests.
Addendum 9/2/2017:
In exploring science, it is important not to cherry pick or ignore papers which fail to support a given hypothesis. So, I am adding another paper to the list of reference and discussing a paper that on the surface would seem to be contradict Dörner’s results. Unfortunately, these papers are behind paywalls and I don’t have copies of them… so I clearly don’t have the details… only the abstracts. Gooren reported in two papers attempts to replicate the LH response and found mixed results, from the ’86 abstract,
“The neuroendocrine response of LH to estrogen administration may be related to sexual dimorphism of the brain, and therefore, homosexual and especially transsexual individuals may differ from heterosexual individuals in their responses. This study failed to find such differences among groups of female heterosexuals, homosexuals, and transsexuals. Specifically, after single dose estrogen administration, all subjects had an initial decline in serum LH levels, followed by a brisk rise of equal magnitude. Among males, the type of response was less uniform. After an initial fall in serum LH levels, the individual responses varied. In 12 of 23 male homosexuals, 10 of 15 male heterosexuals, and all 6 genetic male transsexuals studied, serum LH levels remained below pretreatment levels. In the remaining 11 male homosexuals and 5 of the heterosexuals, serum LH levels increased to values exceeding those before treatment, resembling the response found in the 3 groups of women. Those homosexual and heterosexual men with a rise in serum LH levels to above pretreatment values also had the greatest fall in testosterone levels after estrogen administration, while these same men had the lowest testosterone response to hCG stimulation. I conclude from these results that 1) the similarity of LH responses to estrogen administration in all groups of women studied does not support a theory of brain androgenization as a factor in the establishment of gender identity of sexual orientation; and 2) individual differences in men in the type of LH response to estrogen administration can be satisfactorily explained by endocrine factors, such as Leydig cell function, and need not be related to gender identity, sexual orientation, or other possible causes.”
And in an early ’84 paper,
“In order to test the hypothesis whether there is variation in hormonal levels or response to hormonal manipulation that could permit a distinction between heterosexuals and transsexuals, we designed the following protocol: Six male-to-female (m-to-f) transsexuals, six heterosexual control females and six female-to-male (f-to-m) transsexuals were given estradiol benzoate (E2B) (4.5 micrograms/kg/12 hr) for five days. In the female population, E2B treatment was initiated on day 5 of the menstrual cycle. In all the subjects blood luteinizing hormone (LH) and follicle stimulating hormone (FSH), estradiol-17 beta (E2) and testosterone (T) levels were measured twice daily. Additionally, LH and FSH responses to LHRH (100 micrograms iv) stimulation prior to and on day 5 of the E2B treatment were evaluated. In the m-to-f transsexuals, T levels decreased sharply and progressively during estrogen treatment, along with a fall in LH and FSH levels. The magnitude of the LH and FSH responses to LHRH stimulation also decreased following estrogen administration. In the heterosexual female controls and in the f-to-m transsexuals, estrogen administration increased LH levels to a minimum of 100% above initial values from day 3 onwards. There was no convincing evidence for the existence of a positive estrogen feedback on LH secretion in m-to-f transsexuals. These results contradict some of the reported hypotheses concerning hormonal alterations in these individuals.”
However, in both studies, Gooren made no effort to differentiate between exclusively androphilic (homosexual) transsexuals and gynephilic/bisexual MTF transsexuals as Dörner did. Given the copious evidence from statistical and brain morphology research that differentiates the two types of transwomen, this limits the utility of Gooren’s studies. The only true dissonance between the studies is that Gooren found only a slight difference between homosexual and heterosexual (non-trans) men: 52% of homosexual and 33% of heterosexual men showing a positive LH feedback, while all 6 of the MTF transwomen failed to show any such positive LH feedback.
Although it would appear that this fails to replicate Dörner, I’m astounded that all six of the transwomen failed to show any LH feedback when at least some of the non-transfolk, both homosexual and heterosexual did so. Without knowing which type of transsexual these subjects are, we can’t really say that this fails to replicate Dörner. They could all be gynephilic. There does seem to be small effect size between gay and straight men, but the sample sizes are all too small. Further, I would be very curious as to how Dörner and especially Gooren determined the sexual orientation of their subjects and whether they were exclusively heterosexual and homosexual.
Interesting that all of the FTM transmen showed an exaggerated LH feedback, hmmmm…
Given the Gooren data, small sample as it is, perhaps adding to it another study regarding the difference between heterosexual and homosexual men? We have such a study in Gladue, from the abstract,
“A neuroendocrine component, the positive estrogen feedback effect, thought to be related to sexual orientation and, indirectly, to sexual differentiation, was evaluated in healthy, noninstitutionalized research volunteers. Men and women with a lifelong heterosexual orientation and men with a lifelong homosexual orientation were administered an estrogen preparation known to enhance the concentration of luteinizing hormone in women but not in men. The secretory pattern of luteinizing hormone in the homosexuals in response to estrogen was intermediate between that of the heterosexual men and that of the women. Furthermore, testosterone was depressed for a significantly longer period in the homosexual men than in the heterosexual men. These findings suggest that biological markers for sexual orientation may exist.”
Although, to be fair, this study was also small, but when we add them all together, the direction of the effect seems to be real.
Addendum 9/14/2023: There are a couple other papers that explore the issue of LH & FSH levels in androphilic males including homosexual transsexuals, the first from the same Dörner & Rohde team as some of the papers I cited earlier. From the abstract,
“Plasma basal levels of FSH, LH and total as well as apparent free testosterone were determined in homosexual and heterosexual males. Significantly higher FSH concentrations (mean +/- SD = 6,89+/-5.00 mlU/ml; P less than 0.01) and LH concentrations (28.2+/-30.7 mlU/ml; P less than 0.002) were found in plasma of 50 homosexual males compared with those of 24 or 40 heterosexual males 4.17 +/- 2.34 mlU/ml and 12.6 +/- 7.6 mlU/ml, respectively). Significantly lower free plasma testosterone was observed in 35 homosexual males (10.7 +/- 3.3 ng/100 ml; P less than 0.01) than in 38 heterosexual males (13.3 +/- 4.5 ng/100 ml), whereas total testosterone in plasma of homosexual males (590 +/- 148 ng/100 ml) showed no significant difference in comparison with the heterosexual control group (562 +/- 126 ng/100 ml). The tendency to higher FSH and LH values as well as to lower free testosterone concentrations in plasma compared with the heterosexual control group was more evident for effeminized than for non-effeminized homosexual males. FSH and LH concentrations in plasma of 5 transsexual males were also significantly higher (11.74 +/- 5.06 and 18.3 +/- 3.4 mlU/ml, respectively; P less than 0.02) than those of the heterosexual control group. Our findings may be explained by the possible existence of a prenatal testicular androgen deficiency in homosexual males that is widely compensated by increased gonadotrophin secretion in adult life.”
Note the conjecture regarding prenatal exposure. We can also speculate on the difference between the conventional gay men and the homosexual transsexuals (HSTS). The FSH values for the transsexuals was 11.74 +/- 5.06 vs. 6,89 +/-5.00. This is an effect size of d= 0.96, a large effect. It looks like HSTS and gay men have very different hormonal profiles. Lets look at HSTS vs. heterosexual men with FSH values of 11.74 +/- 5.06 vs. 4.17 +/- 2.34 for an effect size of 1.92, a very large effect size. HSTS look very different than heterosexual men.
But, we can’t cherry pick our data. A year after the above study, another paper by Livingston, et. al., was published in the very same journal that sampled nine (9) homosexuals and found no effect. Who do we trust? First, the second paper had fewer subjects, which may have led to a false negative. The other possibility is that as was noted in the first paper, that there is a difference in subpopulations of homosexual males, specifically between “tops” & “bottoms”. Perhaps tops don’t show the effect found in the first paper?
Further Reading:
References:
Dörner G, Rohde W, Schott G, Schnabl C., “On the LH response to oestrogen and LH-RH in transsexual men.” Experimental Clinical Endrocrinology (1983)
http://www.ncbi.nlm.nih.gov/pubmed/6317420
Dörner G., “Neuroendocrine response to estrogen and brain differentiation in heterosexuals, homosexuals, and transsexuals.” Archives of Sexual Behavior (1988)
http://www.ncbi.nlm.nih.gov/pubmed/3282489?dopt=Abstract
Dörner G, Rohde W, Seidel K, Haas W, Schott GS.”On the evocability of a positive oestrogen feedback action on LH secretion in transsexual men and women.” Endokrinology (1976)
http://www.ncbi.nlm.nih.gov/pubmed/1244197
Gooren L. et al., “Estrogen positive feedback on LH secretion in transsexuality.” Psychoneuroendocrinology (1984)
https://www.ncbi.nlm.nih.gov/pubmed/6436856
Gooren L., “The neuroendocrine response of luteinizing hormone to estrogen administration in heterosexual, homosexual, and transsexual subjects.” Journal of Clinical Endocrinology and Metabolism (1986)
https://www.ncbi.nlm.nih.gov/pubmed/3016021
Gladue A., Green R. Hellman R., “Neuroendocrine response to estrogen and sexual orientation” Science (1984)
https://www.researchgate.net/publication/17097653_Neuroendocrine_response_to_estrogen_and_sexual_orientation
Rohde W, Stahl F, Dörner G. Plasma basal levels of FSH, LH and testosterone in homosexual men. Endokrinologie. 1977;70(3):241-8. https://pubmed.ncbi.nlm.nih.gov/608455/
Livingstone IR, Sagel J, Distiller LA, Morley J, Katz M. The effect of luteinizing hormone releasing hormone (LRH) on pituitary gonadotropins in male homosexuals. Horm Metab Res. 1978 May;10(3):248-9. doi: 10.1055/s-0028-1093445
Comments Off on Brain Power…
Triumph for Whom?
 In a recent popular magazine article, intellectual essayist, Charlotte Allen wrote an extensive and deep exposition on the events of the past 15 years of the increase in visibility of the Transgender community. Encouragingly, it was unflinching in its exploration of not only the pop-psychology, but also the REAL psychology and politics. Of necessity, this also means that she explained about the two type taxonomy, Blanchard’s role in researching it, Bailey’s role in popularizing it… and of the disgraceful behavior of the autogynephilic transwomen who attempted to shout down those who, in their research, came to support the scientific recognition that “late transitioning” transwomen are on the same continuum as transvestites / cross-dressers. Ms. Allen writes,
In a recent popular magazine article, intellectual essayist, Charlotte Allen wrote an extensive and deep exposition on the events of the past 15 years of the increase in visibility of the Transgender community. Encouragingly, it was unflinching in its exploration of not only the pop-psychology, but also the REAL psychology and politics. Of necessity, this also means that she explained about the two type taxonomy, Blanchard’s role in researching it, Bailey’s role in popularizing it… and of the disgraceful behavior of the autogynephilic transwomen who attempted to shout down those who, in their research, came to support the scientific recognition that “late transitioning” transwomen are on the same continuum as transvestites / cross-dressers. Ms. Allen writes,
“Blanchard’s theory is that transgenders fall into two distinct categories whose sexual orientations, interests, choice of careers, and even, to a large extent, social class are violently different from each other. One of those categories he calls “homosexual” transgenders, whose sexual attraction, from childhood to death, is strictly toward members of their own genetic sex. Among males, they’re the extremely effeminate boys who identify as girls in early childhood, play with dolls and other girls’ toys, and shun the rough-and-tumble play typical of boys their age. Studies at Vanderbilt and the University of London have shown that 70 to 80 percent of those trans-children grow out of their trans-identity at puberty and become, simply, gay adolescents and, later, gay adult men. The 20 to 30 percent who do take formal steps toward transitioning, Blanchard believes, are a self-selected group who, thanks to their more delicate looks, can function fairly successfully as women. “They’re people who might be unsuccessful as men,” Blanchard said. — Homosexual transgender men transition early in adulthood, typically during their twenties, Blanchard observed. They account for the vast majority of transgenders in the non-Western world: from the “two-spirits” of indigenous North American tribes, to the fa’afafine of Samoa, to the kathoeys of Thailand who can easily fool Western sex tourists into misidentifying them as women. In those societies there is typically a recognized and thoroughly integrated social niche for men who identify and dress as women. The fa’afafine typically work as secretaries, nannies, and housekeepers—stereotypically female occupations. In that respect, they’re not unlike the flamboyant gay men of Western culture who carved out a recognized social niche for themselves in such occupations as hairdresser, dancer, makeup artist, interior decorator, couturier, and fashion consultant (Queer Eye for the Straight Guy). Boys and men in drag played women’s roles on stage from classical times to the 17th century, and they continue to be popular entertainers for both gays and heterosexuals to this day, as the demographics of the Kit Kat Lounge attest. — By contrast, Blanchard discovered that the predominant form that trangenderism takes in the West today involves men who, as men, have never identified as homosexual in their erotic attractions, but rather as heterosexual, bisexual, or asexual. Those men, his research revealed, tended to make their transitions in their mid-to-late thirties, or even later—at least a full decade on average after the homosexual transgenders did. Furthermore, many of those men were married and fathers before they came out. The paradigm might be travel writer Jan Morris, now 88, who spent the first 46 years of her life as James Morris, the journalist who covered Edmund Hillary’s ascent of Mt. Everest and who fathered five children before undergoing transition surgery in 1972. And many in this heterosexual population—in contrast to the homosexual transgenders on the drag scene—worked in stereotypically hypermasculine professions: They’d been parachutists, Navy SEALs, engineers, policemen, firemen, and high school football coaches. The billionaire philanthropist James Pritzker, who became Jennifer Natalya Pritzker in 2013, in his early sixties, is a retired much-decorated U.S. Army lieutenant colonel with three children by his former wife. “They’ll say that they chose those professions in order to suppress their feelings as females,” Blanchard said. “But no one put a gun to their heads to choose those jobs.” Many late-transitioning transgenders (Jennifer Finney Boylan, for example) insist, contra Blanchard, that they were aware from early childhood that they were born into the wrong body—but Blanchard thinks they aren’t being honest with themselves.”
Ms. Allen then goes on to explain how certain members of the autogynephilic tranwomen’s community took umbridge with Bailey’s attempt at popularizing Blanchard’s work,
“The Man Who Would Be Queen inflamed transgender activists. It did have certain inflammatory aspects. There was the jacket photo of the man in high heels. Blanchard’s coinage “autogynephilia” (extensively used by Bailey in the book), with its connotations of fetishism, deviance, and mental disorder, has never sat well with transgenders. Bailey was even more adamant than Blanchard that autogynephilic transgenders often lied about their erotic fascination with cross-dressing. Furthermore, Bailey observed, drawing on his previous studies, that homosexual transgenders tended to come from lower socioeconomic classes than autogynephiles, and that they tended to have short time-horizons that often led them into streetwalking, shoplifting, and other petty crimes. “Prostitution is the single most common occupation,” Bailey wrote. His book also, perhaps inadvertently, included details about “Cher” that made her real identity quickly discoverable to those in the know: Anjelica Kieltyka, a Chicago transgender woman who, although disagreeing with Bailey about his characterization of her as autogynephilic, had made frequent guest appearances in his classes and had introduced him to other figures in the city’s transgender scene. — Bailey’s book caught the immediate—and hostile—attention of Lynn Conway, now 77, a pioneer of computer-chip design during the 1970s, a longtime engineering professor at the University of Michigan, and a leading transgender activist who figured as one of Time’s “21 Transgender People Who Influenced American Culture” in its May 2014 cover story. Conway was close to Andrea James (both had been patients of Dr. Ousterhout and touted his facial-feminization techniques on their websites). James, best-known for counseling Felicity Huffman, the star of the film Transamerica (2005), on transgender voice and mannerisms, underwent transition surgery in 1996. She and Conway teamed up with Kieltyka, and with Deirdre McCloskey, to make sure that The Man Who Would Be Queen would not receive a respectable academic hearing. McCloskey’s participation in this enterprise seems odd. For one thing, her memoir, Crossing, describes her pre-transition self as having been “sexually aroused” as a young man by accounts of cross-dressing—a classic Blanchard-esque theme.”
She also notes that the science does not support the contention that “late transitioners” have female brains,
“The medical evidence for a mismatch between brains and bodies is ambiguous. The two studies cited most frequently by transgender activists, published in 1995 and 2000, examined the brains of a total of seven male-to-female transgenders and found that a region of the hypothalamus, an almond-shaped area of the brain that controls the release of hormones by the pituitary gland, was female-typical in those brains. But those studies have been criticized for not controlling for the estrogen—which affects the size of the hypothalamus—that most male-to-female transgenders take daily in order to maintain their feminine appearance.”
If I had any serious criticism of her essay, it would be in the way that she hews to the stereotype that transkids, “homosexual transsexuals”, are stereotyped as being prone to becoming petty criminals, prostitutes, and drag performers. I also found her take on the recent improvements in medicine and law regarding the treatment of transchildren and teens to be unsympathetic. She gives one the impression that too many gender variant pre-teens are being pushed into iatrogenic trauma via puberty blockers, etc. While it may be true that autogynephiles may overvalue transition, most transkids and our caregivers are careful not to push children who are more likely to become gay and lesbian adults into wrong paths.
Note: The magazine, The Weekly Standard, from which the above material was drawn is now defunct and the website no longer available.
Comments Off on Triumph for Whom?
A Novel Argument
 A new argument was presented to me just yesterday involving the well documented fact that among those who transitioned as teenagers, far fewer report having experienced autogynephilia. What made the line of argument ironic was that the proponent had started out in absolute denial of any of the science and most especially of the the notion that autogynephilia existed in some transsexuals, “autogynephilia my ass!” However as the debate developed, she presented a novel take on the Nuttbrock data that I presented, to wit that in that study, 82% of self-reported exclusive gynephiles reported sexual arousal to cross-dressing, while only 14% of those who had begun HRT as adolescents (defined in the Nuttbrock study as before one’s 20th birthday) reported such arousal.
A new argument was presented to me just yesterday involving the well documented fact that among those who transitioned as teenagers, far fewer report having experienced autogynephilia. What made the line of argument ironic was that the proponent had started out in absolute denial of any of the science and most especially of the the notion that autogynephilia existed in some transsexuals, “autogynephilia my ass!” However as the debate developed, she presented a novel take on the Nuttbrock data that I presented, to wit that in that study, 82% of self-reported exclusive gynephiles reported sexual arousal to cross-dressing, while only 14% of those who had begun HRT as adolescents (defined in the Nuttbrock study as before one’s 20th birthday) reported such arousal.
Here’s where it gets interesting: In an effort to win ANY point she could, she took the position that I was twisting the data to suit my position… yet in so doing she had to take the position, for her arguments’ logic to work, that autogynephilia is a UNIVERSAL phenomena among MTF transsexuals. I had to laugh privately, since this reversal of her position would obviate all of her previous positions and support some (but not all) of mine. Interestingly, this argument of universal autogynephilia mirrors the argument proposed by another contingent of autogynephilic transwomen, that autogynephilia is also normal and expected in natal women. I find it doubly ironic that there is such an extreme reaction to the two type taxonomy, but from two camps, those that deny any autogynephilia in transwomen, and those who insist that their autogynephilia is just part of being a woman, and thus, all transwomen must also be autogynephilic.
Her argument also starts with several assumptions that are not supported by the data, nor by community observation. She assumed first that HRT in these teens meant “puberty blockers” and that such blockers would preclude an individual from experiencing any sexual arousal. It wasn’t made explicit, but she may also have been making the false assumption that even traditional HRT precludes any sexual arousal. (I’ve heard several “late transitioning” transwomen make this statement, likely due to their own personal experience, while real for these individuals, is neither universal nor inevitable. From casual observation, it seems to occur more frequently in more senior transwomen than younger “late transitioning” transwomen. And from personal conversations with a fair number of transkids, not one had experienced this phenomena.)
So, she explains the significant difference between these adolescents (of whom only one had identified as gynephilic and 7% as bisexual, with the remaining 93% identifying as exclusively androphilic) and the gynephilic (all but one of whom had begun HRT as adults or had never had HRT, and yes, that one individual is in both groups… I couldn’t back her out of the data), as the adolescents not experiencing sexual arousal to cross-dressing due to them not experiencing sexual arousal in general.
So, having convinced herself that she had won her point… she began to crow that I was the one who was not willing to look at reality!!!
Ummm… Not so fast.
Hypothesis were meant to be tested.
I’ve already pointed out the canard that HRT stops sexual arousal in all transwomen. If it did, would we be having sex as often as we do post HRT and SRS, especially transkids? It simply isn’t true. Second, it is extremely unlikely that these youngsters were all on puberty blockers (e.g. Lupron) as it is still a fairly rare protocol. It is typically initiated by well meaning parents bringing their extremely gender dysphoric pre-adolescent children to specialists. While I would wish that all parents were so willing to medically intervene and save their transkid from the damaging effects of endogenous hormones, it is still a rare parent who does so. Most transkids have to fight to get medical help… and many never get parental support, either waiting until they are legally of age, running away early, or getting HRT “on the street” surreptitiously.
Although the Nuttbrock study did not give us the fine detail I would have liked regarding the exact ages which folks started HRT, we know that half of those who identified as androphilic and had started HRT did so before the age of 20. That also means that half did NOT. From other studies, we know that the age of 20 is the median and the mode, that most androphilic transwomen start HRT, not right at puberty, but nearer age 20, showing a Gaussian distribution centered on age 20, with the bulk having started HRT between the ages of 17 and 23 inclusive. This is enough after puberty to have allowed them to experience that first flush of sexual awakening that accompanies the onset of puberty and adolescence.
We know from countless personal narratives of autogynephilia that those early years of adolescence are typically when sexual arousal to autogynephilic imagery, most especially to cross-dressing, stereotypically in women’s lingerie, is the most obvious and intense. Thus, IF these youngsters who began HRT as teens were universally autogynephilic, they would have had ample time to experience it in all of its intensity, before beginning HRT, even if, as was argued, HRT would preclude experiencing it!
Looking further at the Nuttbrock study, only 40% of the self identified exclusively androphilic population had started HRT before age 20. If this argument that HRT in adolescence explains the reduced number reporting autogynephilic arousal to cross-dressing, we would expect that those who did NOT start HRT as an adolescent to report at the same rate as the other sexual orientations. Of those who self-identified as androphilic, all of those, including adolescent onset HRT, adult onset HRT (40%), and not on HRT (20%), the combined population had 23% report autogynephilic arousal to cross-dressing. A little algebra and a calculator will show that those who were NOT adolescent onset HRT were reporting at the rate of 29%, far lower than the 82% of gynephilic transwomen, and even lower than the bisexually identified transwomen who reported at 67%, and the asexual at 66%.
Thus, even if HRT did what my erstwhile debating partner claimed… the data STILL would NOT show that self-reported exclusive androphiles report less than half the incidence of autogynephilic arousal to cross-dressing. We would instead expect the later onset HRT androphiles to report at rates that were at least similar to the bisexual population.
OH… and a note on why I keep using the term “self-reported”: There is, unfortunately for our research purposes, a well documented phenomena of “late transitioning” transwomen misreporting their sexual orientation. It is quite possible, even probable, that the 29% rate of adult onset HRT and no HRT, is from a number of such misreporting older transitioners.
Thus, I’ve outlined my theoretical and evidence based reasons why this novel hypothesis is not supported by the data. Instead, the data supports the two type taxonomy for MTF transsexuality, namely “exclusively androphilic vs. autogynephilic”.
To those who understand the limitations and implications of sociological and psychological studies, I’m sure that the above explication of the data is sufficient. I’m equally certain that to those who are in denial of this research and of the Fruend/Blanchard transsexual taxonomy, what I’ve outlined above will only back them further into their denial.
Comments Off on A Novel Argument
Autogynephilic vs. Even More Autogynephilic
 The $64K question about the Freund/Blanchard two type taxonomy is, “Is it, in fact, taxonic?” That is to say, “Are there in fact two types of MTF transsexuals with each having a different etiology?” The evidence pointing to it is formidable; If one is to try to prove this to be incorrect the evidence to counter it would have to be even more formidable and convincing. A recent paper by Veale attempts and claims to do just that, but fails utterly upon examination, as we shall see. What she has done is to demonstrate that the difference between exclusively gynephilic and bisexual/pseudo androphilic transsexuals is purely dimensional and not taxonic.
The $64K question about the Freund/Blanchard two type taxonomy is, “Is it, in fact, taxonic?” That is to say, “Are there in fact two types of MTF transsexuals with each having a different etiology?” The evidence pointing to it is formidable; If one is to try to prove this to be incorrect the evidence to counter it would have to be even more formidable and convincing. A recent paper by Veale attempts and claims to do just that, but fails utterly upon examination, as we shall see. What she has done is to demonstrate that the difference between exclusively gynephilic and bisexual/pseudo androphilic transsexuals is purely dimensional and not taxonic.
But first, we need to define what is meant by taxonic, and what is not taxonic. As Gangestad explains it,
“Meehl defined a taxon as “a nonarbitrary class whose existence is conjectured as an empirical question, not a mere semantic convenience”. A domain containing taxa is taxonic. Examples include biological sex, biological species, some disease entities (e.g., measles), and some ideological systems in politics or religion (Meehl, 1992). Many taxa are characterized by their causal simplicity. Taxonic domains are more likely than dimensional ones to have specific etiologies, including dichotomous necessary causal factors. For example, infectious diseases are taxa, and their causes consist of specific microbes. (More complex causal processes, such as thresholds and polarization effects, “may also underlie taxa” .) The existence of taxa can be supported either by the demonstration of requisite causal processes or by formal mathematical taxometric methods, which decide whether latent taxa underlie a set of candidate indicators of a conjectured taxon based on numerical relations between them. If so, the formal-numerical taxa that are thereby defined are empirical. Their causal basis must be discovered through additional research, and, thereby, taxometric findings can guide future inquiry into the causes of variation in the domain.”
Turning to the Freund/Blanchard taxonomy, as Veale explains it,
“Blanchard (1989) proposed that there are two distinct types (taxa) of male-to-female (MF) transsexuals and these distinctions are characterized by their sexuality: ‘‘autogynephilic’’ or ‘‘homosexual.’’ According to Blanchard, autogynephilic MF transsexuals are sexually attracted to females (gynephilic), both sexes (bisexual), or neither sex (analloerotic); they are not unusually feminine in childhood; and prior to transitioning often live outwardly successful lives as males, frequently marrying and having children. These MF transsexuals also experience autogynephilia—a term which Blanchard used to refer to ‘‘a male’s propensity to be sexually aroused by the thought of himself as a female’’. Homosexual MF transsexuals are exclusively sexually attracted to males (androphilic), do not experience autogynephilia, are highly feminine in their childhood, do not generally have success with attempts to live in the male role, and tend to present for treatment of their gender dysphoria at a younger age. By splitting MF transsexuals into these two groups based on their sexual orientation, Blanchard 1988,1989) and others (Freund, Steiner, & Chan,1982; Johnson &Hunt, 1990; Nuttbrock et al., 2011a; Smith, van Goozen, Kuiper, & Cohen-Kettenis, 2005) have found evidence for the average differences between these groups that Blanchard proposed. However, these differences do not necessarily imply a typology exists. These results could also have been reached if there was a nontaxonic latent structure with a correlation between the sexual orientation of MF transsexuals and these other differences. Although Blanchard (1985a) found some evidence for a taxonic latent structure of the sexuality of MF transsexuals by obtaining cut-off scores for classifying MF transsexuals into two groups using an earlier version of the taxometric procedures described in this article, he did not specifically test whether the sexuality of MF transsexuals was taxonic or dimensional.”
Veale acknowledges that there are other data that suggest, strongly I would argue, that there are clearly two taxa within the MTF transsexual population. (See FAQ for list of data supporting the two type taxonic structure in MTF transwomen. Also see my blog category “Supporting the Two Type Taxonomy” for essays.) She only directly lists the fraternal birth order effect, which exclusive androphilic transsexuals share with conventional gay men, but NOT autogynephilc transsexuals. But in the literature, we have at least seventeen independent lines of evidence, providing consilience supporting two separate etiologies, and thus two taxa, in MTF transsexuals. This is important, in that Gangestad demonstrated in 2000 that sexual orientation roughly correlated with a latent taxa in the general population. Norris replicated this finding with a different set of correlates in 2015. Thus, there IS a taxonic structure to be considered here… and if so, we need to ask what would a non-taxonic structure among the transsexual population look like?
What is not acknowledged in Veale’s paper, but should be, is that clinical experience shows that autogynephilia also exists in male individuals who do not exhibit gender dysphoria sufficient to motivate them to transition. We call these men, “Cross-Dressers” (CD) or “transvestites” (TV). From long clinical observation, it has been noted that there does not appear to be a sharp line between such autogynephilic individuals, that indeed most autogynephilic transsexuals had careers that exactly match those of CD/TV men before transition. That is also to say, that there appears to be a smooth, dimensional (non-taxonic) spectrum from mildly autogynephilic men to autogynephilic transwomen. Also from societal and clinical observation, we note that exclusively androphilic transwomen population appears to smoothly blend toward feminine gay male “drag queens” to “effeminate” gay men, with no obvious gaps in the populations. That is also to say, that there appears to be a smooth, dimensional (non-taxonic) spectrum from mildly feminine gay men (bottoms) to exclusively androphilic transwomen. If Veale is right, than that would imply that heterosexual cross-dressers are members of the same taxon as feminine gay men. Although I don’t believe this to be correct, it has a certain superficial theoretical appeal in that cross-dressers and autogynephilic transwomen both claim that their behavior is related to a ‘feminine essence’. Hypothesis were meant to be tested. I will come back to this after further examination of Veale’s study below.
In order to test whether Blanchard’s hypothesis is correct, she used statistical procedures proposed by Meehl; MAXCOV and MAMBAC. I’m not going to even try to explain how these work. But there are a few points to using these techniques that should be noted as they will figure prominently in the reasons why Veale failed to demonstrate that Blanchard’s hypothesis is incorrect. First, the bare minimum number of subjects in the study needs to be 300. The second is that the minimum number of subjects in the smaller of the two suspected taxons must be at least 30, and that the measures used to differentiate the suspected taxons must be valid. Veale collected the needed 300 transwomen, but she failed to reach the needed minimum of 30 exclusive androphilic transswomen; worse, she failed to differentiate between bisexual/psuedo-androphilic and exclusely androphilic transwomen, using an invalid measure, as Lawrence showed in her critique of the Veale study,
In this commentary on Veale’s article, which incorporates a reanalysis of some of her data, I will argue that her critique of Blanchard’s typology was invalid, because:
1. Veale’s measures of sexual orientation and autogynephilia were not well constructed, which probably interfered with the accurate identification of participants’ sexual orientations and artificially lowered estimates of their autogynephilic arousal.
2. In her taxometric analysis,Veale employed several measures that were unrelated to the defining features of Blanchard’s typology. This rendered her analysis invalid as a confirmation or disconfirmation of Blanchard’s typology: Whatever typology Veale was examining, it was not Blanchard’s typology.
3. Even if Veale had used well-constructed measures of sexual orientation and autogynephilia and had conducted her taxometric analysis utilizing the defining features of Blanchard’s typology, the number of genuinely androphilic participants she was able to recruit—probably 18 (5.8 %) at most, and possibly even fewer—was too small to be reliably detectable through taxometric analysis. If the structure of Veale’s data appears to be dimensional rather than taxonic, this is because her participants consisted almost exclusively of only one of the two MtF transsexual types: nonhomosexuals (or nonandrophiles).
I’m far less concerned about the construction of Veale’s novel measures of autogynephilia, as almost any measures that meet the minimum required correlations with Blanchard’s Core Autogynephilic Scale would do for a taxonometric analysis. But the real deal killer to her study was that she incorrectly included so many clearly non-exclusively androphilic transwomen in the “exclusively androphilic” category. How do we know this? My suspicions were first raised by the low effect size (d=0.37) regarding core autogynephilia and sexual orientation. From Veale:
Sexual Orientation: Androphilic Nonandrophilic
. (n=36) (n=272)
Core Value (SD)
autogynephilia 14.08 (14.66) 19.00 (12.21)
The values are nearly the same, especially considering the very large range of scores. These score differences strike me as being very much like the differences in reported autogynephilia found between exclusive gynephiles and bisexuals and asexuals in previous studies, rather than the larger differences between non-androphilies and androphiles. If a large number, more than half, of the putative androphiles were in fact bisexual and asexual, I would expect the scores to look exactly like this. Lawrence also suspected this to be the case as she corresponded with Veale to obtain the raw data used to classify the subjects into sexual orientation categories. From this, she demonstrated that at least half (and likely more) of the 36 putatively ‘androphilic’ subjects were decidedly bisexual instead,
“I have reorganized these supposedly androphilic informants into three groups, based on their self-reported gynephilia before age 16 (‘‘degree to which, until the age of 16, you felt sexually attracted to females’’; Veale, 2005, p. 129) and within each of these groups, based on their self-reported androphilia before age 16 (‘‘degree to which, until the age of 16, you felt sexually attracted to males’’; Veale, 2005, p. 129). My reasoning is that some of Veale’s purported androphiles were probably actually pseudo-androphiles or bisexuals—that is, their fundamental sexual attraction was towards females, but at some point they developed a secondary sexual interest in males as a consequence of their autogynephilic sexuality—and that the easiest way to detect these persons would be to look for informants who reported moderate or greater levels of gynephilia or very low levels of androphilia or both during adolescence.
First, consider the 12 informants with Reference numbers 1–12 in Table 1: All reported sexual attraction to females at least ‘‘occasionally’’ before age 16, even though their total Androphilia scores were high and their total Gynephilia scores were low. Not surprisingly, however, their mean Core Autogynephilia score—24.0—was also high, compared to a mean of only 19.0 in the 272 informants whom Veale categorized as nonandrophilic. Moreover, the mean Autogynephilic Interpersonal Fantasy score of these 12 informants—10.9—was also high, compared to a mean of only 8.2 in Veale’s 272 nominally nonandrophilic informants. Based on their early history of gynephilia and their high mean Core Autogynephilia and Autogynephilic Interpersonal Fantasy scores, I believe there is good reason to conclude that these 12 informants were actually pseudo-androphilic or bisexual, rather than genuinely androphilic as Veale alleged.
Next, consider the six informants with Reference numbers 13–16 and 24–25 in Table 1. Although these informants reported little sexual attraction to females before age 16, they also reported ‘‘rarely’’ or ‘‘never’’ experiencing sexual attraction to males before age 16; this suggests that they developed significant sexual attraction to males rather late in life. The mean total Androphilia score of these six informants—11.8—was also somewhat lower than that of the rest of the nominally androphilic group that reported little gynephilia (Reference numbers 17–23 and 26–36; n=18), with a mean total Androphilia score of 16.4. Again not surprisingly, the mean Core Autogynephilia score of these 6 informants was 18.3, nearly equal to that of the 272 nominally nonandrophilic informants, 19.0, and substantially higher than that of the rest of the nominally androphilic group that reported little gynephilia (n=18), 6.1. However, the mean Autogynephilic Interpersonal Fantasy score of these six informants, 6.5, was similar to that of the rest of the nominally androphilic group that reported little gynephilia (n=18), 6.9. Although the case here is not quite as strong as for the 12 informants who reported significant gynephilia before age 16, I believe that most or all of these 6 informants who rarely or never experienced sexual attraction to males before age 16 were also pseudo-androphilic or bisexual, rather than genuinely androphilic as Veale alleged.
There are also a few other specific supposed androphiles whose androphilia seems questionable. For example, consider the informant with Reference number 30,whose total Gynephilia score of 8 reflected her being aroused by females in her current sexual fantasies ‘‘almost all the time,’’ currently feeling sexually attracted to females ‘‘occasionally,’’ and having been conscious of sexual arousal to females while in physical contact with them ‘‘occasionally’’: Given her Core Autogynephilia score of 37 and Autogynephilic Interpersonal Fantasy score of 13, one might suspect that she was actually pseudo-androphilic or bisexual. Or consider the informants with Reference numbers 18 and 26, whose total Androphilia scores of 9 both reflected the identical pattern of only ‘‘occasional’’ attraction to males before age 16 and currently, sexual arousal to males in their current sexual fantasies only ‘‘sometimes,’’ and having been conscious of sexual arousal to males while in physical contact with them only ‘‘occasionally’’ : Here one might suspect mild pseudo-androphilic or bisexual ideation in fundamentally analloerotic individuals.”
From this analysis, Lawrence contends (and I wholeheartedly concur) that 18 of these individuals were not exclusive androphiles, and three more were very likely not. Personally, I would say that these additional three are definitely not. Given that this would leave, at best, only 18, and likely less, androphilic individuals, the number is definitely too low to be detected as a taxon using the techniques in Veale’s study. Remember also that for taxonometric analysis, that the scales must be valid. Failing to differentiate psuedo-bisexual from exclusively androphilic demonstrated that the sexual orientation scale Veale employed was most definitely not valid. Further, given that most of the putatively androphilic individuals were in fact non-androphilic, Veale’s study does successfully demonstrate that the various non-androphilic categories are dimensional and non-taxonic, supporting Blanchard’s hypothesis.
Lawrence pointed out that Veale’s method of obtaining her subjects was prone to ascertainment bias. Simply put, one does not find androphilic transwomen at autogynephilically dominated venues such as online forums and support groups. Veale herself recommended that a “more representative” sample would be needed for future studies.
Suggestions for future studies.
Hypothesis were meant to be tested.
Lawrence has criticized Veale’s use of her novel “attraction to feminine males” and to “attraction to transgender fiction” scales. Veale has previously shown an interest in developing these as a means of exploring autogynephilic sexuality, as the former is based on the observation that many autogynephiles are gynandromorphophilic and that many autogynephiles like to write and share autogynephilically inspired erotica. While I think these are worthy areas to explore, I have to concur with Lawrence that these are not the appropriate scales to use for future taxonometric analysis tests in MTF transwomen. Instead I would highly recommend using Blanchard’s Autogynephilia Scale and the Childhood Gender Non-conformity (CGN) Scale from Gangestad, as I believe that these will show that the Freund/Blanchard categorization of MTF transsexuals is taxonic with the two types being autogynephilic and “homosexual”. My prediction is that there will be a very high negative correlation between CA and CGN scales that will show a taxonic structure over sexual orientation. Sexual orientation should be based on pre-SRS behavior, not on self-reported identity, which has been shown repeatedly, to be unreliable and subject to social desirability bias in autogynephilic transwomen.
For a dichotomous separation of exclusively androphilic and non-androphilic transwomen, I recommend a multi-factorial sieve. First, if they self report being gynephilic, bisexual, or asexual: believe them, they are non-androphilic. Next, of the remainder, ask these two questions, “Are you now, or have you ever been, married to a woman?” and “Have you ever fathered a child?”; if yes, then they are non-androphilic. (Lawrence previously used marital status to exclude bisexuals from androphiles.) Finally, of the remainder, survey their actual sexual history with these two items, “Estimate how many times you have had sexual intercourse with a woman” and “Estimate how many times you had receptive sexual contact with a man’s penis before SRS (excluding cross-dressed/feminized males)”. A validation study may be needed to determine appropriate cut-offs for the first question. I would be tempted to use “zero” (0), but that may be overly aggressive… but I would be very surprised if genuinely exclusive androphiles had more than a nominal experimental number, say three at most. The second question supports the first, and also allows discrimination of celibate analloerotic individuals. I expect that for androphilic transwomen, older than say 2o, the number of sexual contacts with men will be greatly higher than the number of vaginal intercourse experiences.
For a continuous androphilic scale, (moderately) free from social desirability bias, take the number of vaginal intercourse experiences and subtract it from the number of sexual encounters with men. This scale will be negative for sexually experienced gynephiles and positive for androphiles.
Evidence for taxonic structure in MTF transsexuals includes that showing that autogynephilia is found in only one of the putative taxa and can be shown to be a causitive etiological factor not shared with the exclusively androphilic taxon.
References:
Gangestad, Steven W.; Bailey, J. Michael; Martin, Nicholas G., “Taxometric analyses of sexual orientation and gender identity”
Journal of Personality and Social Psychology, Vol 78(6), Jun 2000, 1109-1121. doi: 10.1037/0022-3514.78.6.1109
Norris, et al, “Homosexuality as a Discrete Class”
Psychological Science, Oct 2015
doi: 10.1177/0956797615598617
Jaimie F. Veale, “Evidence Against a Typology: A Taxometric Analysis of the Sexuality of Male-to-Female Transsexuals” Archives of Sexual Behavior
DOI 10.1007/s10508-014-0275-5
Anne A. Lawrence, “Veale’s (2014) Critique of Blanchard’s Typology Was Invalid” Archives of Sexual Behavior
DOI 10.1007/s10508-014-0383-2
Comments Off on Autogynephilic vs. Even More Autogynephilic
The More Things Change…
…The More They Stay the Same
![]() Recently, the Diagnostic & Statistics Manual, usually called by its initials, the DSM, of the American Psychiatric Association, considered by most physicians and even researchers, to be the single most important document on psychiatric conditions, was updated. The new DSM V has an updated section on transsexual/transgender diagnoses and description. In several ways, it was both an improvement, and a set back, for transfolk.
Recently, the Diagnostic & Statistics Manual, usually called by its initials, the DSM, of the American Psychiatric Association, considered by most physicians and even researchers, to be the single most important document on psychiatric conditions, was updated. The new DSM V has an updated section on transsexual/transgender diagnoses and description. In several ways, it was both an improvement, and a set back, for transfolk.
First, the improvement and a bit of history. Decades ago, during the days that in my history class I called, ‘The Clinic Years”, the days when nearly all North American and European transfolk were dependent upon organized clinics for SRS, often associated with universities such as John Hopkins and Stanford, they typically excluded people that they thought fell outside of the “classic transsexual” diagnoses. If you were a heterosexual MTF, and especially if you admitted to being sexually aroused by cross-dressing, you were not “transsexual” you were simply a “transvestite”, period. But one clinic dispensed with this restriction, led by Norman Fisk, M.D. Dr. Fisk coined a new term and a description of a syndrome that he described as “liberalizing” the allowable indications for HRT and SRS, “Gender Dysphoria”. As Anne Lawrence described it:
“Fisk (1974a, b; Laub & Fisk, 1974) distinguished several types of male patients who sought sex reassignment at the Stanford University gender program. He used the term gender dysphoria syndrome, rather than transsexualism, to refer to these patients’ diagnosis. In Fisk’s typology, the number of recognized typological categories and their exact names varied slightly from one article to another. It appears that persons in only three of Fisk’s typological categories, however, were considered appropriate candidates for SRS in the Stanford program (Laub & Fisk, 1974): classic transsexualism of Benjamin (a reference to Benjamin, 1966), effeminate homosexuality, and transvestism. Only patients in these three categories, for example, were selected for inclusion in a follow-up descriptive study of applicants to the Stanford program (Dixen, Maddever, Van Maasdam, & Edwards, 1984); consequently, only these categories are included in Table 2. Other typological categories described by Fisk included persons with psychosis, extreme sociopathy and psychopathy, and inadequate/schizoid personality (1974b; Laub & Fisk, 1974). Classic MtF transsexualism was characterized by onset in early childhood, life-long feminine behavior, exclusive androphilia, absence of sexual arousal with cross-dressing, and perhaps a disinterest in genital sexuality (Fisk, 1974a; Laub & Fisk, 1974). Effeminate homosexuality progressing to gender dysphoria syndrome was characterized by androphilia, episodic nonerotic cross-dressing, and onset of gender dysphoria in adulthood (Laub & Fisk, 1974). Transvestism progressing to gender dysphoria syndrome was characterized by erotic arousal with cross-dressing, gynephilia, and onset of gender dysphoria in adulthood (Laub & Fisk, 1974).”
Here, I get to share a bit of my personal history, in that I was diagnosed as “transsexual” by Dr. Fisk in early 1975, when I was 17 years old. So I have cherished memories of having had a grand total of six hours talking to him… but in those six hours, I got a glimpse into the mind that cut through the confusion of the differing types of candidates for sex reassignment and sought to offer such liberalized palliative medicine. Yet, I can also tell you from those six hours, two of which were in the company of my parents (one hour each, separately, given that they were in the process of an unhappy divorce) that Fisk was a VERY skeptical man. He dug into my history, sexuality, and aspirations with a vengeance. I’m betting he did so with everyone. In fact, the very first half hour spent with him, I got the very distinct impression that he was ready to believe that every word out of my mouth would be a lie. At the time, I couldn’t understand why that should be, given that at 17, I was very naïve about the state of the on going debate in medical and scientific circles… and especially unknowing of how autogynephilic transwomen were lying to the clinics, including to Dr. Fisk. I think it was meeting my mother, and hearing her very bitter, angry, and even hateful confirmation of my personal history and behavior since early childhood that led him to believe me. I share this to put some color on Fisk’s support of liberalizing the diagnoses with a new inclusive term and syndrome. Dr. Fisk supported HRT and SRS for “older transitioners” not because he believed their narritives, but because he recognized that they were in just as much of a quandary and in pain as the younger androphilic, non-autogynephilic, MTF transkids. He was a hero.
So, back to the DSM. Looking at the history of changes in the DSM over the decades, one can detect an undercurrent of the tides, the ebb and flow, between pragmatic science based medicine and political / social positioning. When trans issues were first described in the DSM, it was “Transsexualism”, from the DSM, as described by Anne Lawrence (personal communication),
“Transsexualism was characterized as a “heterogeneous disorder” (p. 261), and four subtypes were recognized:
“The disorder is subdivided according to the predominant prior sexual history, which is coded in the fifth digit [e.g., 302.53] as 1 = asexual, 2 = homosexual (same anatomic sex), 3 = heterosexual (opposite anatomic sex), and 0 = unspecified.” (p. 262)
This section goes on to explain that “In the third group, ‘heterosexual,’ the individual claims to have had an active heterosexual life.” (p. 262)
In the section “Predisposing Factors (p. 263), the DSM-III recognizes that “Some cases of Transvestism evolve into Transsexualism.” Finally, in the section on “Differential Diagnosis” (p. 263), it is noted that “In both Transvestism and Transsexualism there may be cross-dressing. However, in Transvestism that has not evolved into Transsexualism there is no wish to be rid of one’s own genitals.”
The diagnostic criteria for Transsexualism (pp. 263-264) are admirably brief and uncomplicated:
1. Sense of discomfort and inappropriateness about one’s anatomic sex.
2. Wish to be rid of one’s own genitals and to live as a member of the other sex.
3. The disturbance has been continuous (not limited to periods of stress) for at least two years.
4. Absence of physical intersex or genetic abnormality.
5. Not due to another mental disorder, such as Schizophrenia.”
But later, the DSM changed the name of the disorder to “Gender Identity Disorder” which causes a distortion in therapy for all concerned because it focuses on “identity” on not on the source of their disorder. It is even more of a distortion of the description of the etiological processes. This was somewhat improved in the DSM-IV-TR, in that it used sexual orientation specifiers and an explanation of autogynephilia as a phenomena and an etiological origin of late transitioning transwomen’s late developing “gender identity disorder”.
Now, four decades later, the DSM has finally caught up to Dr. Fisk by using the term Gender Dysphoria Disorder.
This is the good news, in that the diagnoses speaks directly to the actual ‘pain’ of the condition, rather than to the totally inaccurate and misleading concept of a Gender Identity Disorder. It is also good in that the history of the term goes back to Fisk’s papers that specifically describe how it incudes autogynephilic males. However, the bad news is that the DSM no longer adequately describes autogynephilia and how it is etiologically related to gender dysphoria… and worse, still places too much emphasis on the concept of gender identity mismatch as the cause of gender dysphoria in autogynephilic transwomen, rather than the result of autogynephilic gender dysphora, as the science shows. However, this reliance on “gender identity” is now euphemistically cloaked in the term “experienced / expressed gender”.
There are other problems with it, as Lawrence explains,
“…MtF and FtM transsexuals and the clinicians who treat them have traditionally recognized that a profound sense of ‘‘wrong embodiment’’—distress related to biologic sex and sexed body characteristics—is almost always a prominent feature of transsexualism and GD, in part because such wrong embodiment usually makes it difficult or impossible to ‘‘live and be accepted as a member of the opposite sex’’ (World Health Organization, 1992, p. 365). This “trapped in the wrong body’’ metaphor is not mere poetic rhetoric but offers an authentic description of transsexuals’ subjective experience. … This understanding has been largely, if not quite completely, abandoned in the DSM-5. It has been replaced by an emphasis on ‘‘assigned gender,’’ a change that seems to have occurred entirely for political and social reasons, not for scientific or clinical ones. In the DSM-5, all the clinical indicators of GD—even those that refer to biologic sex characteristics—are now conceptualized as being clinically relevant only by virtue of their evincing an ‘‘incongruence between one’s experienced/expressed gender and assigned gender’’ (APA, 2013, p. 452; the neologism ‘‘experienced/expressed gender’’ is essentially synonymous with ‘‘gender identity’’). In this formulation, the principal thing that feels wrong in transsexualism and GD is not one’s biologic sex but one’s assigned gender. This same perspective is, as we shall see, also reflected in the Subwork group members’ implicit position that effective treatment of transsexualism and GD does not require changing sexed body characteristics but only changing nominal gender assignment, as evidenced by their contention that undergoing gender transition—the only absolute criterion for which is ‘‘full-time living in the desired gender’’ (APA, 2013, p. 453)—automatically results in loss of the GD diagnosis.”
I’m not sure that this was their intent… but taken literally, one’s GD diagnoses, and thus any medical necessity justification for performing, and certainly third-party financing of, sex reassignment surgery or much needed ongoing therapeutic support services, is eliminated the moment that one is socially living as, or perceived as being, the opposite sex! This is a bizarre result of the latest rewrite, one that Lawrence contends was done at the behest of “late transitioning” transsexuals themselves, in an effort to rid themselves of the stigma of a psychiatric diagnoses… one that is ended the moment that they transition full time. Hopefully, the next interim revision will correct this mistake.
(Note 9/11/2014: This essay has been edited to correct an error with respect to the history of the DSM III, thanks Anne.)
Further Reading:
References:
Fisk, N. (1974a). Gender dysphoria syndrome: The conceptualization that liberalizes indications for total gender reorientation and implies a broadly based multi-dimensional rehabilitative regimen [Editorial comment]. Western Journal of Medicine, 120, 386–391. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1130142/
Fisk, N. (1974b). Gender dysphoria syndrome (the how, what, and why of a disease). In D. R Laub & P. Gandy (Eds.), Proceedings of the Second Interdisciplinary Symposium on Gender Dysphoria Syndrome (pp. 7–14). Stanford, CA: Stanford University Press.
Laub, D. R., & Fisk, N. M. (1974). A rehabilitation program for gender dysphoria syndrome by surgical sex change. Plastic and Reconstructive Surgery, 53, 388–403.
Lawrence, A. A. (2010). Sexual orientation versus age of onset as bases for typologies (subtypes) of gender identity disorder in adolescents and adults. Archives of Sexual Behavior, 39, 514-545.
Lawrence, A., “Gender Assignment Dysphoria in the DSM-5”, Archives of Sexual Behavior, DOI 10.1007/s10508-013-0249-z
Comments Off on The More Things Change…
One Size Fits All…
“One Size Fits All”… and other lies… Or “Why it matters”
Beyond mere scientific curiosity, there are other compelling reasons why we need to recognize the two types of transsexuals as distinct and having separate etiologies and life arcs. Research on appropriate treatment protocols is confounded when we don’t segregate them. Treatment itself is less effective and potentially counter productive when using the wrong protocol, or when using a ‘one-size-fits-all’, middle of the road protocol. Finally, we dishonor who we truly are when we don’t recognize the differences.
Consider that our present protocols for treating gender dysphoric teenagers is a muddled attempt to reconcile the experiences of autogynephilic (AGP) MTF adults and young HSTS, both FtM and the minority MTF feminine androphilic. If MTF “late transitioners” did not exist at all, would we be as concerned about attempting to delay puberty as a reversible treatment, given that transkid teenagers rarely have regrets or negative outcomes when given full HRT instead? But we do have AGP teens for whom transition and HRT are not warranted, who go on to live very satisfactory lives as heterosexual cross-dressers. If we fully recognized and diagnosed the two populations separately as teens and young adults, we would have very different treatment protocols. We could access AGP teens as to the level of gender dysphoria distress and stability and provide puberty blockers for them, will allowing HSTS to proceed to HRT.
Consider also, that our present protocols for adults have a requirement that a candidate for sex reassignment surgery have been living full time as their new sex before surgery, as though that fact somehow guaranteed that post-operative regret would not occur… or that surgery is simply providing genitals that match the social gender in which the client is living. Neither is the case! Sex reassignment surgery may, in fact I would strongly argue, is not contra-indicated by still living as one’s birth gender. If we didn’t have the example of transkids for whom living in their new gender and sex reassignment surgery are intimately linked, would we have this requirement?
It’s possible that without the existence and example of feminine androphilic MTF HSTS, whom many AGP transwomen attempt to emulate closely, Western Society might not have developed and accepted the medical category “transsexual”. But now that we have decades of data that show that AGP transwomen are the majority, and that that majority does find improvement (at least palliatively in most cases), should we not review the assumptions that were made in the early years that only “true” transsexuals, those who needed to both live full time and rid themselves of their unused genitalia, are the only ones who would benefit from HRT and sex reassignment surgery?
Might the original purpose of the “real life test” have been not simply to reduce post-operative regret, but was (wrongly it turned out) a means of weeding out “transvestites” (autogynephiles) who were thought to not be able to pass such tests?
I would argue strongly that there is absolutely no association with living full time and lack of post-op regret. Further, I would argue that for many AGP individuals, the “real life test” requirement is needlessly socially and professionally destructive. How many AGP individuals would have benefited from HRT and/or sex reassignment surgery to rid themselves of the anatomic-autogynephilically induced gender dysphoria without having needed to live as women full time? How many of them would have found a life of integration far better? A life of the “bi-gender” individual, one who is professionally and socially a man during the weekday, but socially and sexually a woman during the evenings and weekends? Our present protocols discount these people. They must make a choice between no surgery, or up-ending their professional and social lives. How many individuals have been falsely declared to have been treatment failures because after SRS, they “de-transitioned”, having obtained their true objective and now free to live their lives without the so called “Standards of Care” dictating their lives?
In therapy, the two types have very different needs. First, most HSTS do not need therapy. But our Standards of Care (at least as practiced, if not as written) require that one have been evaluated by a therapist or psychiatrist before any medical interventions. Why should a feminine androphilic HSTS be treated differently than any other young woman? Why should she need to get “permission” before having breast implants and not a natal female? Could it be because she is conflated with autogynephiles for whom many practitioners are concerned may regret such interventions? What of FtMs? Many natal females have breast reduction surgery, but aren’t required to obtain letters from therapists before hand. I argue that our protocols for transgendered people have been developed with experience of autogynephilic MTFs, for whom such evaluations and therapies are recommended.
Autogynephiles suffer from severe shame and guilt. Many cross-dressers report a cycle of purging, throwing away their feminine wardrobes in self-loathing. Many autogynephilic transwomen have had similar histories, but rarely discuss this or other autogynephilic experiences with their therapists, rightly or wrongly, assuming that the therapist is wearing their “gate-keeper” hat and might not “OK” them for HRT or SRS if that were known. Because both the AGP transsexual community and their therapists fail to face head on the issue of autogynephilia, this shame and guilt remains untreated. Instead, the client is left with secret denial or other defenses. Because she has not faced her own autogynephilia, she may stigmatize others who are processing their autogynephilic experiences, shutting down group therapy discussions on the matter and even attacking other transwomen in public forums, harming the transgendered community at large. Worse, for the individual, is that the shame, guilt, and denial are lurking in her psyche, waiting for some dark moment to come crashing to the fore, when her defenses fail, and the reality of her autogynephilic sexuality come crashing upon her. The result may be catastrophic, perhaps even fatal.
The suicide rate among transgendered people is well known to be high. Medical intervention is intended to alleviate suffering; but because the two types are not fully differentiated and because autogynephilia is not openly acknowledged, AGP transsexuals remain at risk for mental heath problems, especially depression and anxiety.
The two types should never be grouped together for therapy. The two types have completely different goals and concerns. Further, there is a very unfortunate tendency for AGP transwomen to attempt to model themselves upon transkids, to the point where they edit and even confabulate histories to match those of HSTS, interfering with the therapeutic process. Worse, this process of editing and confabulation puts pressure on their families, in effect gas lighting wives and mothers, who are required to acquiesce and either accept the false history or end their relationships. Conversely, HSTS are very often uncomfortable around autogynephiles, leading them to emotionally, and even physically, to withdraw from the group. Comparing themselves and their experiences to the other type is also very damaging to their self-images, for differing reasons for each type.
Would HRT protocols be different if the types were not conflated? Consider MPA, a synthetic progestin. It is well known to sharply reduce libido. Many AGP transwomen find their autogynephilic arousal intrusive and unwelcome. For them, MPA may be a welcome addition to estradiol… or even alone. But for feminine androphilic MTF HSTS transkids, reduction in libido is never desired. For them, micronized progesterone is a better addition to estradiol.
Would protocols be different for the two regarding fertility? Many AGP transwomen are already natural parents, having sired children with their wives or girlfriends. But what of the young AGP transwomen who have not yet sired children? Would they not benefit from banking their sperm before beginning HRT? Would the same be right for MTF HSTS transkids? I would argue not. First, it would mean that they would have to wait for spermatogenesis, which would also mean damaging exposure to endogenous testosterone. Better to begin HRT without ever being able to generate sperm. Further, for the slightly older (post-pubertal) transitioning HSTS transkid, consider the psychological implications for her future husband… surely if they elect to pursue surrogacy, it should be his sperm, not hers?
For these, and yet other practical reasons, it matters that the two types be officially, scientifically, medically, and socially recognized as distinct.
Further Reading:
Essay on the need for segregated group therapy.
Comments Off on One Size Fits All…

Comments Off on Are Drag Queens and Homosexual Transsexuals In The Same Spectrum?